

In vivo validation of 4D flow MRI for assessing the hemodynamics of portal hypertension
- PMID: 23148034
- PMCID: PMC4000737
- DOI: 10.1002/jmri.23906
In vivo validation of 4D flow MRI for assessing the hemodynamics of portal hypertension
Abstract
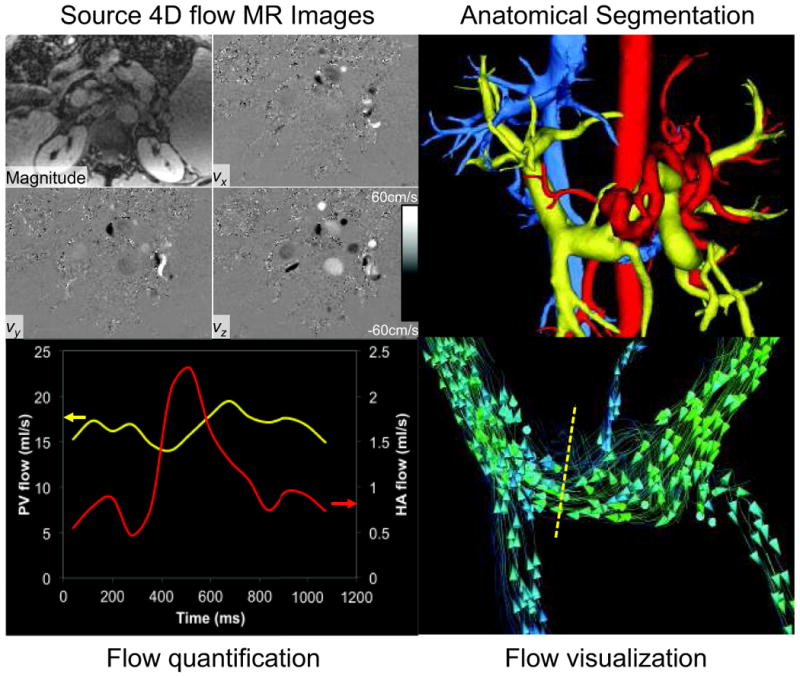
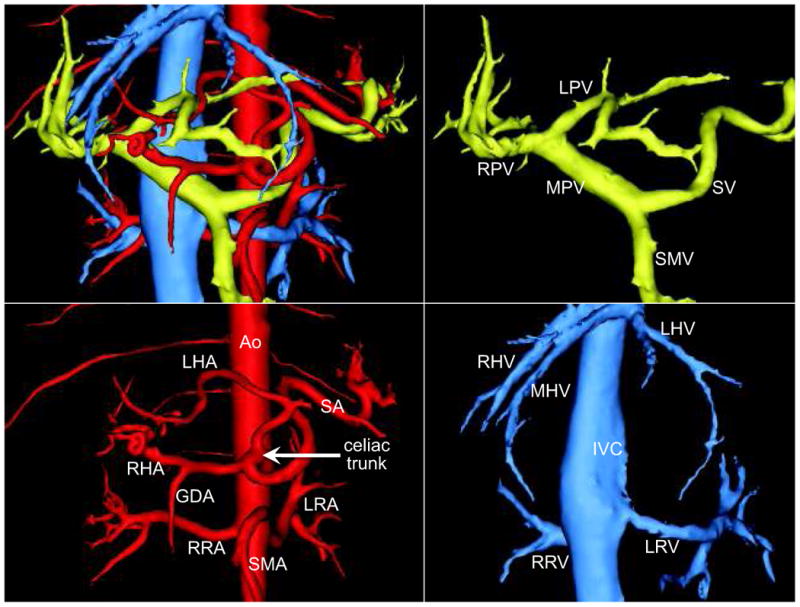
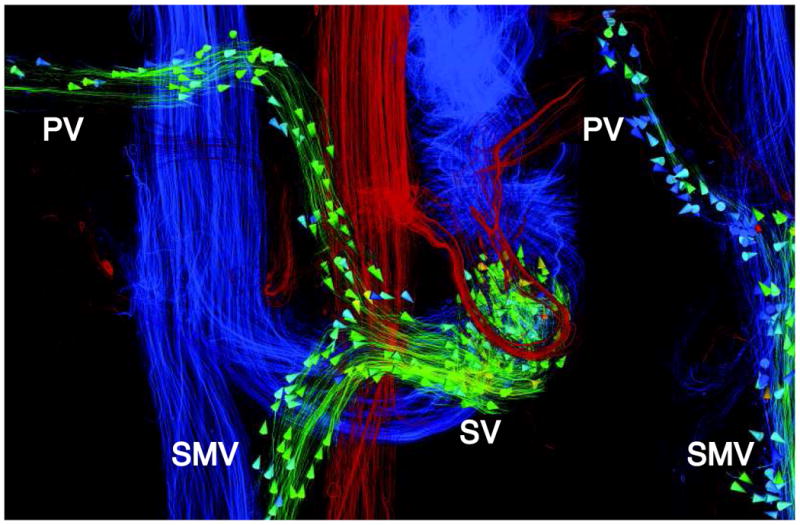
Purpose: To implement and validate in vivo radial 4D flow MRI for quantification of blood flow in the hepatic arterial, portal venous, and splanchnic vasculature of healthy volunteers and patients with portal hypertension.
Materials and methods: Seventeen patients with portal hypertension and seven subjects with no liver disease were included in this Health Insurance Portability and Accountability Act (HIPAA)-compliant and Institutional Review Board (IRB)-approved study. Exams were conducted at 3T using a 32-channel body coil with large volumetric coverage and 1.4 mm isotropic true spatial resolution. Using postprocessing software, cut-planes orthogonal to vessels were used to quantify flow (L/min) in the hepatic and splanchnic vasculature.
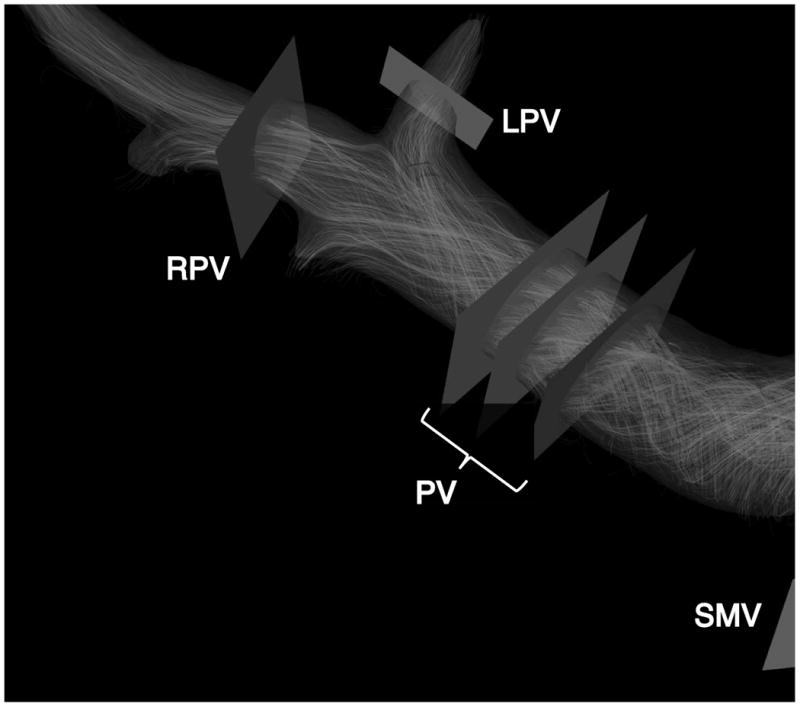
Results: Flow quantification was successful in all cases. Portal vein and supraceliac aorta flow demonstrated high variability among patients. Measurements were validated indirectly using internal consistency at three different locations within the portal vein (error = 4.2 ± 3.9%) and conservation of mass at the portal confluence (error = 5.9 ± 2.5%) and portal bifurcation (error = 5.8 ± 3.1%).
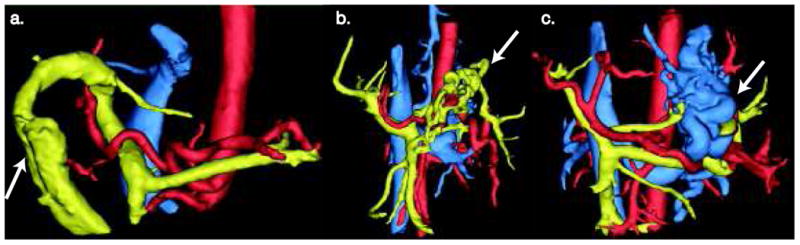
Conclusion: This work demonstrates the feasibility of radial 4D flow MRI to quantify flow in the hepatic and splanchnic vasculature. Flow results agreed well with data reported in the literature, and conservation of mass provided indirect validation of flow quantification. Flow in patients with portal hypertensions demonstrated high variability, with patterns and magnitude consistent with the hyperdynamic state that commonly occurs in portal hypertension.
Copyright © 2012 Wiley Periodicals, Inc.
Figures



References
-
- Centers for Desease Control and Prevention. 2009
-
- Bhathal PS, Grossman HJ. Reduction of the increased portal vascular resistance of the isolated perfused cirrhotic rat liver by vasodilators. J Hepatol. 1985;1(4):325–337. - PubMed
-
- Zardi EM, Dobrina A, Uwechie V, et al. Postmeal portal flow variations in HCV-related chronic hepatitis and liver cirrhosis with and without hyperdynamic syndrome. In Vivo. 2008;22(4):509–512. - PubMed
-
- Moller S, Hobolth L, Winkler C, Bendtsen F, Christensen E. Determinants of the hyperdynamic circulation and central hypovolaemia in cirrhosis. Gut. 2011;60(9):1254–1259. - PubMed
-
- Burkart DJ, Johnson CD, Ehman RL, Weaver AL, Ilstrup DM. Evaluation of portal venous hypertension with cine phase-contrast MR flow measurements: high association of hyperdynamic portal flow with variceal hemorrhage. Radiology. 1993;188(3):643–648. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
