

Heterogeneity in outcomes of treated HIV-positive patients in Europe and North America: relation with patient and cohort characteristics
- PMID: 23148105
- PMCID: PMC3535877
- DOI: 10.1093/ije/dys164
Heterogeneity in outcomes of treated HIV-positive patients in Europe and North America: relation with patient and cohort characteristics
Abstract
Background: HIV cohort collaborations, which pool data from diverse patient cohorts, have provided key insights into outcomes of antiretroviral therapy (ART). However, the extent of, and reasons for, between-cohort heterogeneity in rates of AIDS and mortality are unclear.
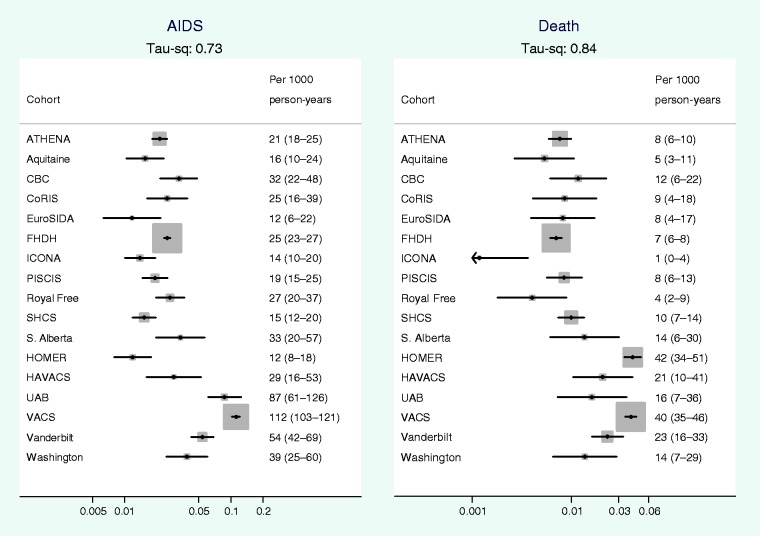
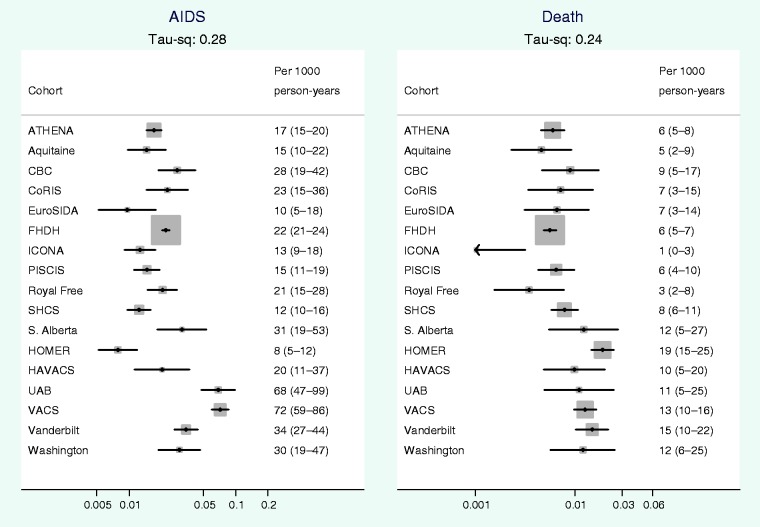
Methods: We obtained data on adult HIV-positive patients who started ART from 1998 without a previous AIDS diagnosis from 17 cohorts in North America and Europe. Patients were followed up from 1 month to 2 years after starting ART. We examined between-cohort heterogeneity in crude and adjusted (age, sex, HIV transmission risk, year, CD4 count and HIV-1 RNA at start of ART) rates of AIDS and mortality using random-effects meta-analysis and meta-regression.
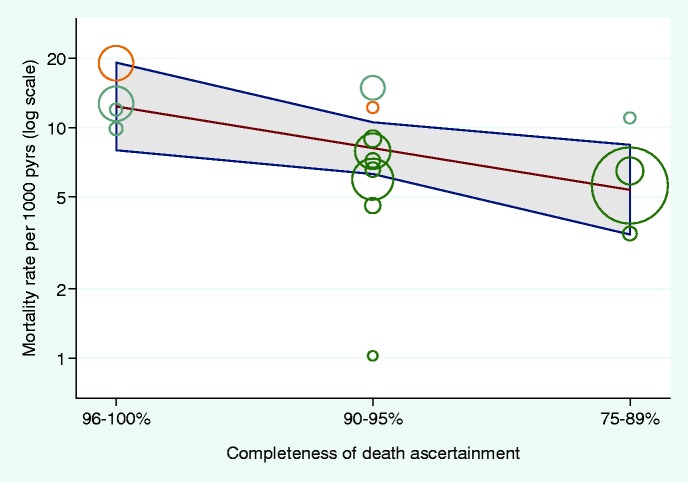
Results: During 61 520 person-years, 754/38 706 (1.9%) patients died and 1890 (4.9%) progressed to AIDS. Between-cohort variance in mortality rates was reduced from 0.84 to 0.24 (0.73 to 0.28 for AIDS rates) after adjustment for patient characteristics. Adjusted mortality rates were inversely associated with cohorts' estimated completeness of death ascertainment [excellent: 96-100%, good: 90-95%, average: 75-89%; mortality rate ratio 0.66 (95% confidence interval 0.46-0.94) per category]. Mortality rate ratios comparing Europe with North America were 0.42 (0.31-0.57) before and 0.47 (0.30-0.73) after adjusting for completeness of ascertainment.
Conclusions: Heterogeneity between settings in outcomes of HIV treatment has implications for collaborative analyses, policy and clinical care. Estimated mortality rates may require adjustment for completeness of ascertainment. Higher mortality rate in North American, compared with European, cohorts was not fully explained by completeness of ascertainment and may be because of the inclusion of more socially marginalized patients with higher mortality risk.
Figures
References
-
- Egger M, May M, Chene G, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospectivestudies. Lancet. 2002;360:119–29. - PubMed
-
- Mocroft A, Vella S, Benfield TL, et al. Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet. 1998;352:1725–30. - PubMed
-
- Babiker A, Darbyshire J, Pezzotti P, et al. Short-term CD4 cell response after highly active antiretroviral therapy initiated at different times from seroconversion in 1,500 seroconverters. J Acquir Immune Defic Syndr. 2003;32:303–10. - PubMed
-
- Sabin CA, Smith CJ, D’Arminio MA, et al. Response to combination antiretroviral therapy: variation by age. AIDS. 2008;22:1463–73. - PubMed
-
- Law M, Friis-Moller N, Weber R, et al. Modelling the 3-year risk of myocardial infarction among participants in the Data Collection on Adverse Events of Anti-HIV Drugs (DAD) study. HIV Med. 2003;4:1–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
