

Clinical management of SIADH
- PMID: 23148195
- PMCID: PMC3474650
- DOI: 10.1177/2042018812437561
Clinical management of SIADH
Abstract
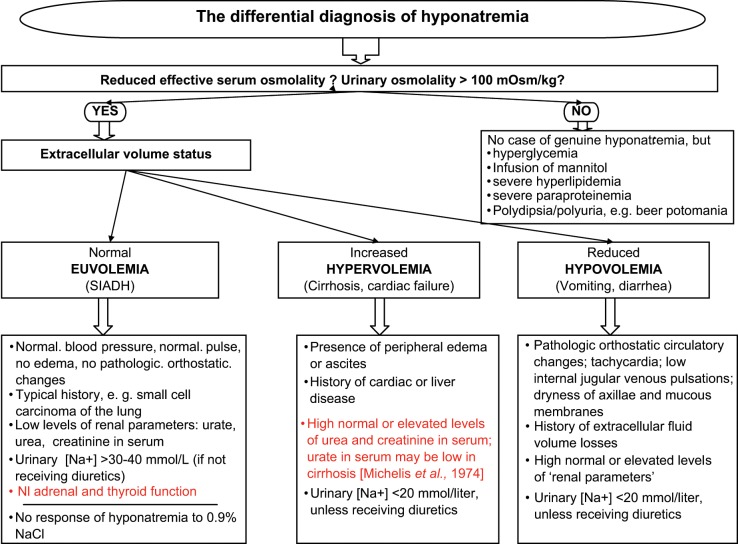
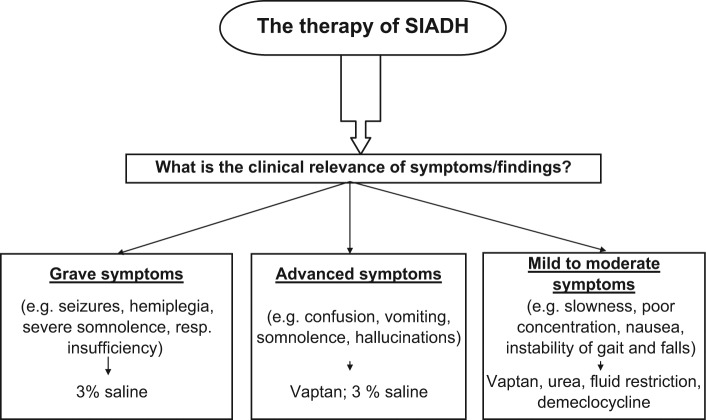
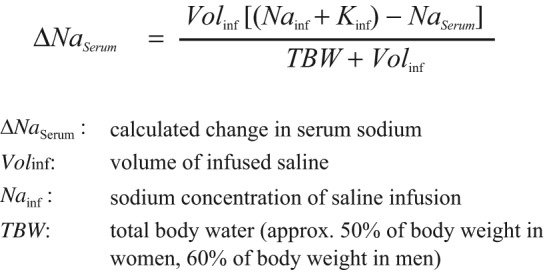
Hyponatremia is the most frequent electrolyte disorder and the syndrome of inappropriate antidiuretic hormone secretion (SIADH) accounts for approximately one-third of all cases. In the diagnosis of SIADH it is important to ascertain the euvolemic state of extracellular fluid volume, both clinically and by laboratory measurements. SIADH should be treated to cure symptoms. While this is undisputed in the presence of grave or advanced symptoms, the clinical role and the indications for treatment in the presence of mild to moderate symptoms are currently unclear. Therapeutic modalities include nonspecific measures and means (fluid restriction, hypertonic saline, urea, demeclocycline), with fluid restriction and hypertonic saline commonly used. Recently vasopressin receptor antagonists, called vaptans, have been introduced as specific and direct therapy of SIADH. Although clinical experience with vaptans is limited at this time, they appear advantageous to patients because there is no need for fluid restriction and the correction of hyponatremia can be achieved comfortably and within a short time. Vaptans also appear to be beneficial for physicians and staff because of their efficiency and reliability. The side effects are thirst, polydipsia and frequency of urination. In any therapy of chronic SIADH it is important to limit the daily increase of serum sodium to less than 8-10 mmol/liter because higher correction rates have been associated with osmotic demyelination. In the case of vaptan treatment, the first 24 h are critical for prevention of an overly rapid correction of hyponatremia and the serum sodium should be measured after 0, 6, 24 and 48 h of treatment. Discontinuation of any vaptan therapy for longer than 5 or 6 days should be monitored to prevent hyponatremic relapse. It may be necessary to taper the vaptan dose or restrict fluid intake or both.
Keywords: antidiuretic hormone; hyponatremia; syndrome of inappropriate antidiuretic hormone secretion; vaptans.
Conflict of interest statement
Peter Gross has been an investigator in vaptan studies of Wyeth-Ayerst, Astellas, Sanofi and Otsuka. He has given presentations and been on an advisory board for Otsuka.
Figures
References
-
- Abraham W.T., Shamshirsaz A.A., McFann K., Oren R.M., Schrier R.W. (2006) AQuaretic effects of lixivaptan, an oral, non-peptide, selective V2 receptor vasopressin antagonist, in New York association functional class II and III chronic heart failure patients. J Am Coll Cardiol 47: 1615–1621 - PubMed
-
- Adrogué H.J. (2005) Consequences of inadequate management of hyponatremia. Am J Nephrol 25: 240–249 - PubMed
-
- Adrogué H.J., Madias N.E. (2000) Hyponatremia. N Engl J Med 342: 1581–1589 - PubMed
-
- Anderson R.Z., Chung H.M., Kluge R., Schrier R.W. (1985) Hyponatremia: a prospective analysis of its epidemiology and the pathogenetic role of vasopressin. Ann Intern Med 102: 164–168 - PubMed
-
- Annane D., Decaux G., Smith N. (2009) Efficacy and safety of oral conivaptan, a vasopressin-receptor antagonist, evaluated in a randomized, controlled trial in patients with euvolemic or hypervolemic hyponatremia. Am J Med Sci 337: 28–36 - PubMed
LinkOut - more resources
Full Text Sources
