

Myocardial structural associations with local electrograms: a study of postinfarct ventricular tachycardia pathophysiology and magnetic resonance-based noninvasive mapping
- PMID: 23149263
- PMCID: PMC3581804
- DOI: 10.1161/CIRCEP.112.970699
Myocardial structural associations with local electrograms: a study of postinfarct ventricular tachycardia pathophysiology and magnetic resonance-based noninvasive mapping
Abstract
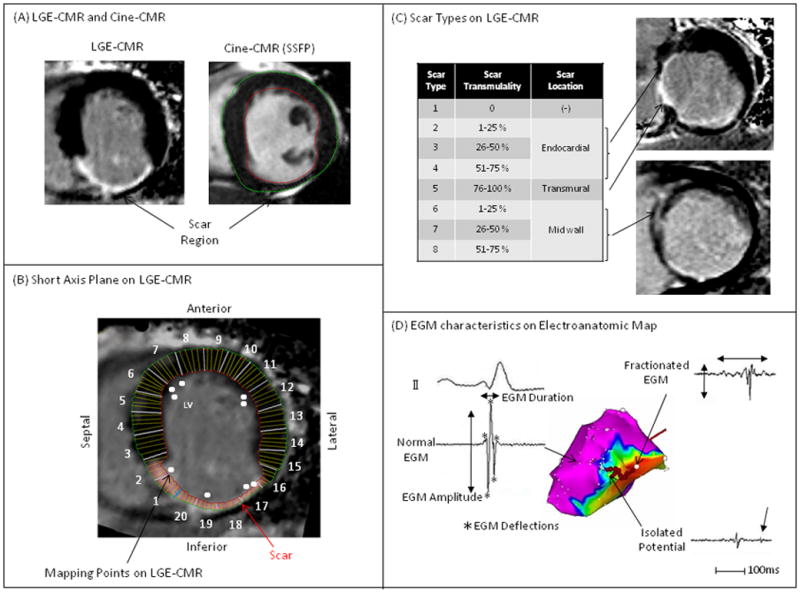
Background: The association of scar on late gadolinium enhancement cardiac magnetic resonance (LGE-CMR) with local electrograms on electroanatomic mapping has been investigated. We aimed to quantify these associations to gain insights regarding LGE-CMR image characteristics of tissues and critical sites that support postinfarct ventricular tachycardia (VT).
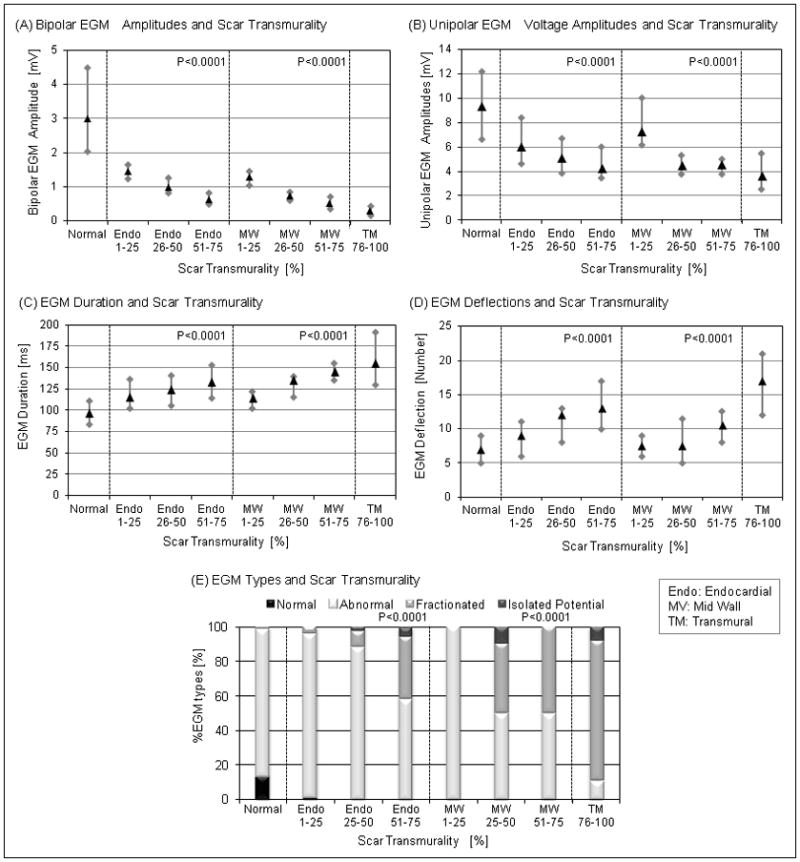
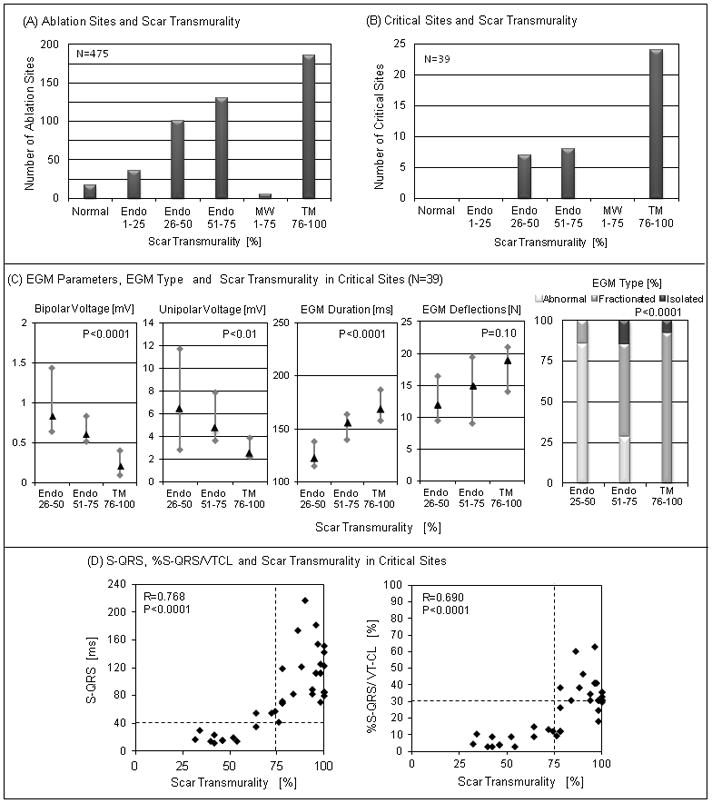
Methods and results: LGE-CMR was performed in 23 patients with ischemic cardiomyopathy before VT ablation. Left ventricular wall thickness and postinfarct scar thickness were measured in each of 20 sectors per LGE-CMR short-axis plane. Electroanatomic mapping points were retrospectively registered to the corresponding LGE-CMR images. Multivariable regression analysis, clustered by patient, revealed significant associations among left ventricular wall thickness, postinfarct scar thickness, and intramural scar location on LGE-CMR, and local endocardial electrogram bipolar/unipolar voltage, duration, and deflections on electroanatomic mapping. Anteroposterior and septal/lateral scar localization was also associated with bipolar and unipolar voltage. Antiarrhythmic drug use was associated with electrogram duration. Critical sites of postinfarct VT were associated with >25% scar transmurality, and slow conduction sites with >40 ms stimulus-QRS time were associated with >75% scar transmurality.
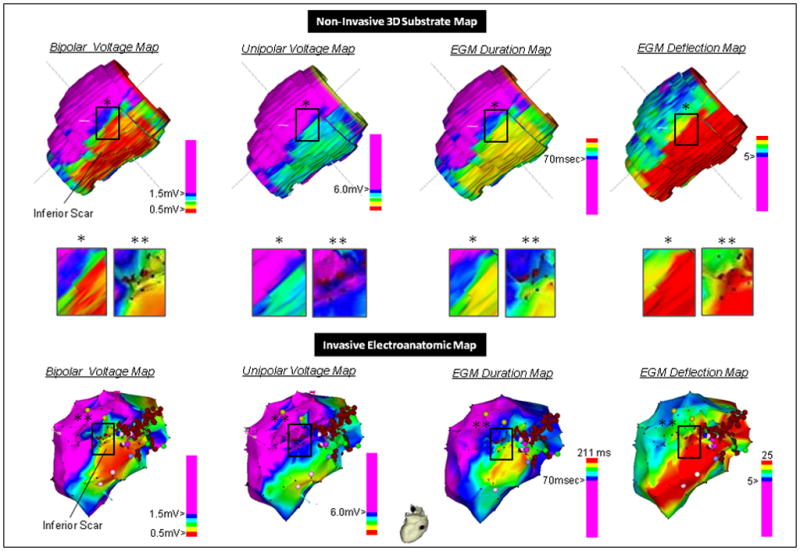
Conclusions: Critical sites for maintenance of postinfarct VT are confined to areas with >25% scar transmurality. Our data provide insights into the structural substrates for delayed conduction and VT and may reduce procedural time devoted to substrate mapping, overcome limitations of invasive mapping because of sampling density, and enhance magnetic resonance-based ablation by feature extraction from complex images.
Conflict of interest statement
Figures
References
-
- Stevenson WG, Khan H, Sager P, Saxon LA, Middlekauff HR, Natterson PD, Wiener I. Identification of reentry circuit sites during catheter mapping and radiofrequency ablation of ventricular tachycardia late after myocardial infarction. Circulation. 1993;88:1647–1670. - PubMed
-
- Hsia HH, Lin D, Sauer WH, Callans DJ, Marchlinski FE. Anatomic characterization of endocardial substrate for hemodynamically stable reentrant ventricular tachycardia: Identification of endocardial conducting channels. Heart Rhythm. 2006;3:503–512. - PubMed
-
- Stevenson WG, Sager PT, Natterson PD, Saxon LA, Middlekauff HR, Wiener I. Relation of pace mapping qrs configuration and conduction delay to ventricular tachycardia reentry circuits in human infarct scars. J Am Coll Cardiol. 1995;26:481–488. - PubMed
-
- Bogun F, Good E, Reich S, Elmouchi D, Igic P, Lemola K, Tschopp D, Jongnarangsin K, Oral H, Chugh A, Pelosi F, Morady F. Isolated potentials during sinus rhythm and pace-mapping within scars as guides for ablation of post-infarction ventricular tachycardia. J Am Coll Cardiol. 2006;47:2013–2019. - PubMed
-
- Estner HL, Zviman MM, Herzka D, Miller F, Castro V, Nazarian S, Ashikaga H, Dori Y, Berger RD, Calkins H, Lardo AC, Halperin HR. The critical isthmus sites of ischemic ventricular tachycardia are in zones of tissue heterogeneity, visualized by magnetic resonance imaging. Heart Rhythm. 2011;8:1942–1949. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
