

Interventions to improve influenza and pneumococcal vaccination rates among community-dwelling adults: a systematic review and meta-analysis
- PMID: 23149531
- PMCID: PMC3495928
- DOI: 10.1370/afm.1405
Interventions to improve influenza and pneumococcal vaccination rates among community-dwelling adults: a systematic review and meta-analysis
Abstract
Purpose: Influenza and pneumococcal vaccination rates remain below national targets. We systematically reviewed the effectiveness of quality improvement interventions for increasing the rates of influenza and pneumococcal vaccinations among community-dwelling adults.
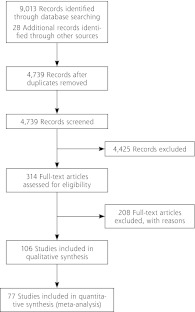
Methods: We included randomized and nonrandomized studies with a concurrent control group. We estimated pooled odds ratios using random effects models, and used the Downs and Black tool to assess the quality of included studies.
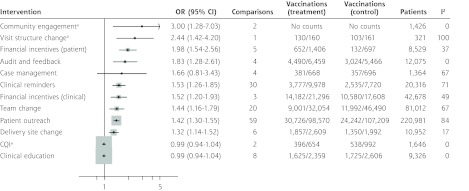
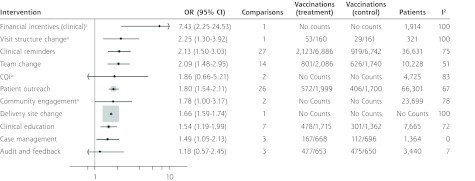
Results: Most studies involved elderly primary care patients. Interventions were associated with improvements in the rates of any vaccination (111 comparisons in 77 studies, pooled odds ratio [OR] = 1.61, 95% CI, 1.49-1.75), and influenza (93 comparisons, 65 studies, OR = 1.46, 95% CI, 1.35-1.57) and pneumococcal (58 comparisons, 35 studies, OR = 2.01, 95% CI, 1.72-2.3) vaccinations. Interventions that appeared effective were patient financial incentives (influenza only), audit and feedback (influenza only), clinician reminders, clinician financial incentives (influenza only), team change, patient outreach, delivery site changes (influenza only), clinician education (pneumococcus only), and case management (pneumococcus only). Patient outreach was more effective if personal contact was involved. Team changes were more effective where nurses administered influenza vaccinations independently. Heterogeneity in some pooled odds ratios was high, however, and funnel plots showed signs of potential publication bias. Study quality varied but was not associated with outcomes.
Conclusions: Quality improvement interventions, especially those that assign vaccination responsibilities to nonphysician personnel or that activate patients through personal contact, can modestly improve vaccination rates in community-dwelling adults. To meet national policy targets, more-potent interventions should be developed and evaluated.
Conflict of interest statement
Conflicts of interest: authors report none.
Figures
References
-
- Thompson MG, Shay DK, Zhou H, et al. Centers for Disease Control and Prevention (CDC) Estimates of deaths associated with seasonal influenza—United States, 1976-2007. MMWR Morb Mortal Wkly Rep. 2010;59(33):1057-1062 - PubMed
-
- Thompson WW, Shay DK, Weintraub E, et al. Influenza-associated hospitalizations in the United States. JAMA. 2004;292(11):1333-1340 - PubMed
-
- Pulido M, Sorvillo F. Declining invasive pneumococcal disease mortality in the United States, 1990-2005. Vaccine. 2010;28(4):889-892 - PubMed
-
- Nuorti JP, Whitney CG, Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices Updated recommendations for prevention of invasive pneumococcal disease among adults using the 23-valent pneumococcal polysaccharide vaccine (PPSV23). MMWR Morb Mortal Wkly Rep. 2010;59(34):1102-1106 - PubMed
-
- Advisory Committee on Immunization Practices Prevention of Pneumococcal Disease: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 1997;46(RR-8):1-31 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical