

Embryonic exposure to propylthiouracil disrupts left-right patterning in Xenopus embryos
- PMID: 23150524
- PMCID: PMC3545537
- DOI: 10.1096/fj.12-218073
Embryonic exposure to propylthiouracil disrupts left-right patterning in Xenopus embryos
Abstract
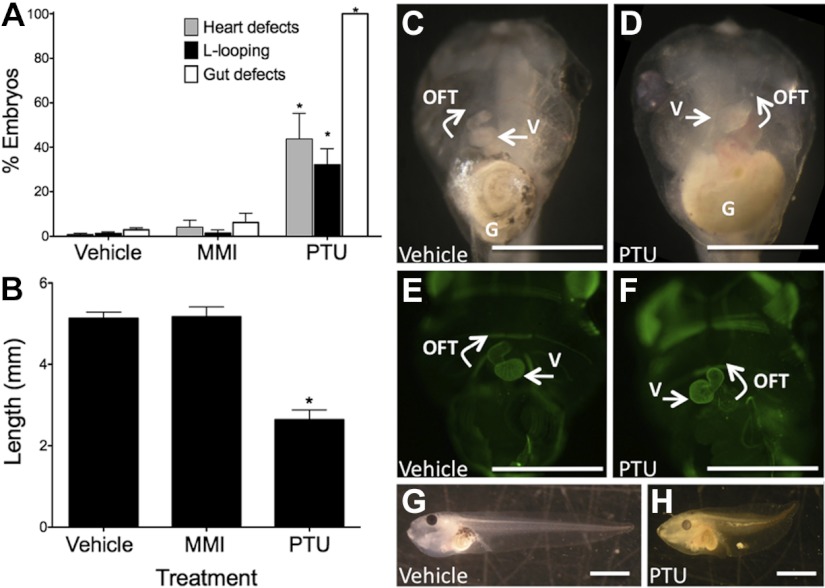
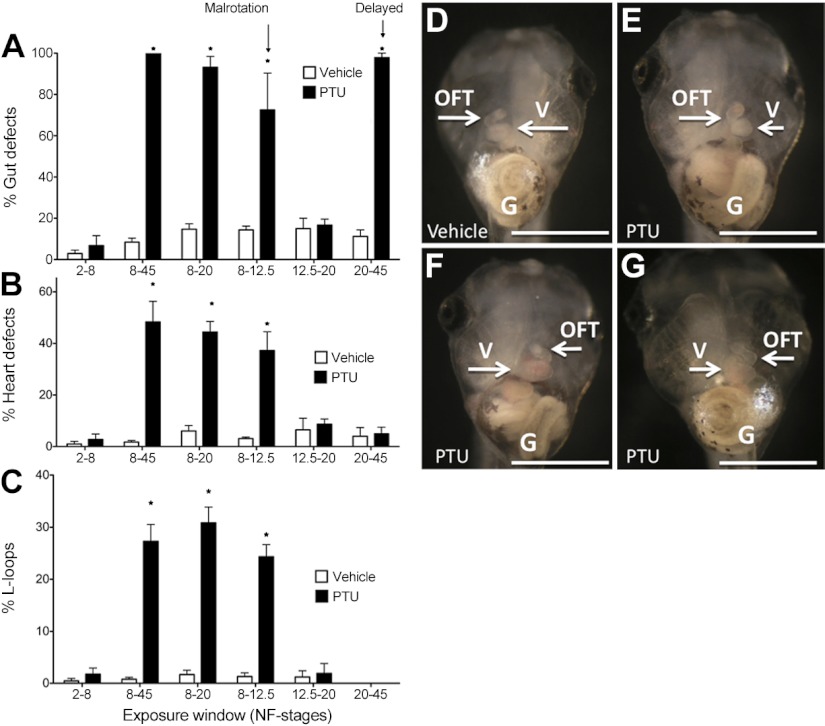
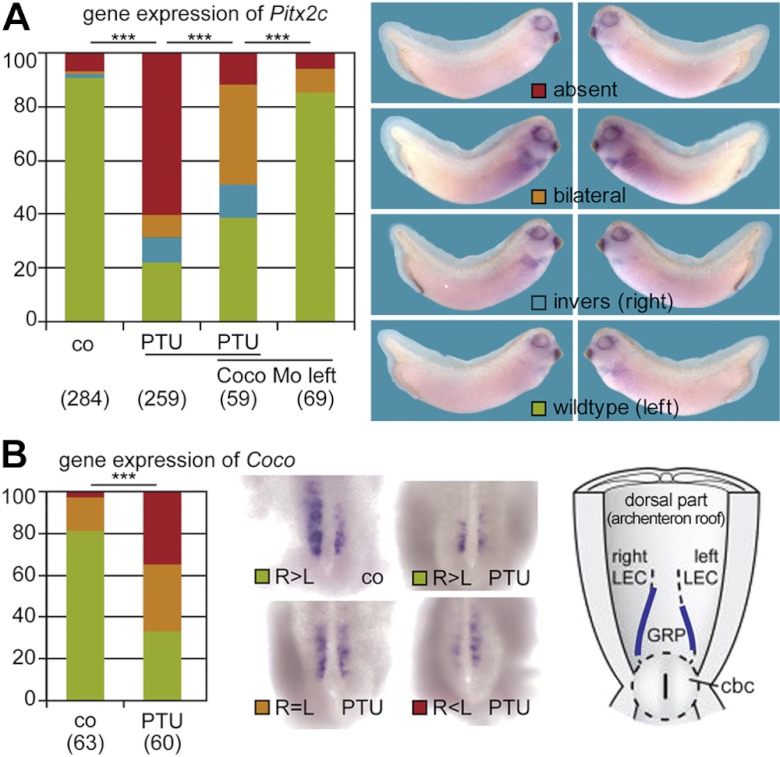
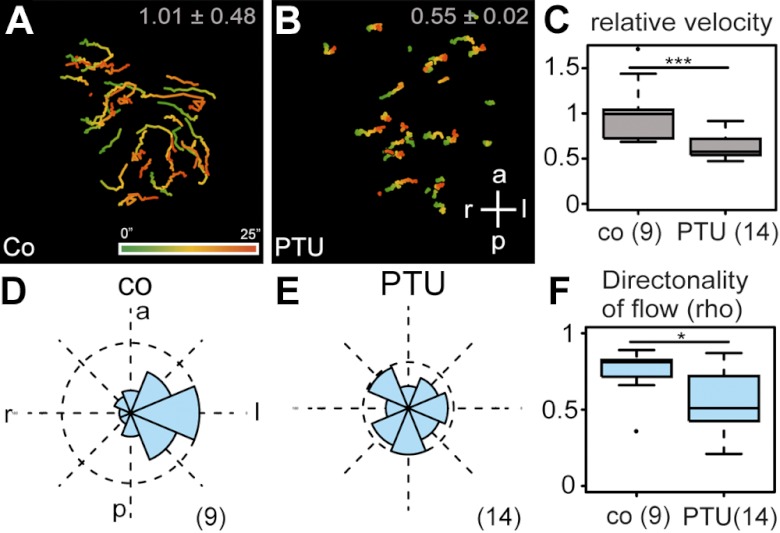
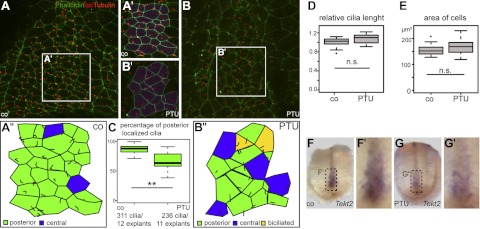
Antithyroid medications are the preferred therapy for the treatment of Graves' disease during pregnancy. Propylthiouracil (PTU) is favored over methimazole (MMI) due to potential teratogenic concerns with MMI. This study was to determine the teratogenic potential of MMI and PTU using a validated Xenopus tropicalis embryo model. Embryos were exposed to 1 mM PTU (EC(50)=0.88 mM), 1 mM MMI, or vehicle control (water) from stages 2 to 45. Treated embryos were examined for gross morphological defects, ciliary function, and gene expression by in situ hybridization. Exposure to PTU, but not MMI, led to cardiac and gut looping defects and shortening along the anterior-posterior axis. PTU exposure during gastrulation (stage 8-12.5) was identified as the critical period of exposure leading to left-right (LR) patterning defects. Abnormal cilia polarization, abnormal cilia-driven leftward flow at the gastrocoel roof plate (GRP), and aberrant expression of both Coco and Pitx2c were associated with abnormal LR symmetry observed following PTU exposure. PTU is teratogenic during late blastula, gastrulation, and neurulation; whereas MMI is not. PTU alters ciliary-driven flow and disrupts the normal genetic program involved in LR axis determination. These studies have important implications for women taking PTU during early pregnancy.
Figures
Similar articles
-
Evaluation of developmental toxicity of propylthiouracil and methimazole.Birth Defects Res B Dev Reprod Toxicol. 2014 Aug;101(4):300-7. doi: 10.1002/bdrb.21113. Epub 2014 Jun 30. Birth Defects Res B Dev Reprod Toxicol. 2014. PMID: 24980470 Free PMC article.
-
Propylthiouracil is teratogenic in murine embryos.PLoS One. 2012;7(4):e35213. doi: 10.1371/journal.pone.0035213. Epub 2012 Apr 18. PLoS One. 2012. PMID: 22529993 Free PMC article.
-
Comparison of single daily dose of methimazole and propylthiouracil in the treatment of Graves' hyperthyroidism.Clin Endocrinol (Oxf). 2004 Jun;60(6):676-81. doi: 10.1111/j.1365-2265.2004.02032.x. Clin Endocrinol (Oxf). 2004. PMID: 15163329 Clinical Trial.
-
Toxicological considerations for antithyroid drugs in children.Expert Opin Drug Metab Toxicol. 2011 Apr;7(4):399-410. doi: 10.1517/17425255.2011.557068. Epub 2011 Feb 17. Expert Opin Drug Metab Toxicol. 2011. PMID: 21323607 Review.
-
The propylthiouracil dilemma.Curr Opin Endocrinol Diabetes Obes. 2012 Oct;19(5):402-7. doi: 10.1097/MED.0b013e3283565b49. Curr Opin Endocrinol Diabetes Obes. 2012. PMID: 22820213 Review.
Cited by
-
Risk of congenital anomalies associated with antithyroid treatment during pregnancy: a meta-analysis.Clinics (Sao Paulo). 2015 Jun;70(6):453-9. doi: 10.6061/clinics/2015(06)12. Epub 2015 Jun 1. Clinics (Sao Paulo). 2015. PMID: 26106966 Free PMC article. Review.
-
Evaluation of developmental toxicity of propylthiouracil and methimazole.Birth Defects Res B Dev Reprod Toxicol. 2014 Aug;101(4):300-7. doi: 10.1002/bdrb.21113. Epub 2014 Jun 30. Birth Defects Res B Dev Reprod Toxicol. 2014. PMID: 24980470 Free PMC article.
-
Notch signaling induces either apoptosis or cell fate change in multiciliated cells during mucociliary tissue remodeling.Dev Cell. 2021 Feb 22;56(4):525-539.e6. doi: 10.1016/j.devcel.2020.12.005. Epub 2021 Jan 4. Dev Cell. 2021. PMID: 33400913 Free PMC article.
-
Mink1 regulates spemann organizer cell fate in the xenopus gastrula via Hmga2.Dev Biol. 2023 Mar;495:42-53. doi: 10.1016/j.ydbio.2022.11.010. Epub 2022 Dec 23. Dev Biol. 2023. PMID: 36572140 Free PMC article.
-
Hyperthyroidism in pregnancy: evidence and hypothesis in fetal programming and development.Endocr Connect. 2021 Feb;10(2):R77-R86. doi: 10.1530/EC-20-0518. Endocr Connect. 2021. PMID: 33444223 Free PMC article. Review.
References
-
- Mestman J. H. (1998) Hyperthyroidism in pregnancy. Endocrinol. Metab. Clin. North Am. 27, 127–149 - PubMed
-
- Glinoer D. (1998) Thyroid hyperfunction during pregnancy. Thyroid 8, 859–864 - PubMed
-
- Fantz C. R., Dagogo-Jack S., Ladenson J. H., Gronowski A. M. (1999) Thyroid function during pregnancy. Clin. Chem. 45, 2250–2258 - PubMed
-
- Abalovich M., Amino N., Barbour L. A., Cobin R. H., De Groot L. J., Glinoer D., Mandel S. J., Stagnaro-Green A. (2007) Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 92, S1–S47 - PubMed
-
- Okosieme O. E., Marx H., Lazarus J. H. (2008) Medical management of thyroid dysfunction in pregnancy and the postpartum. Expert Opin. Pharmacother. 9, 2281–2293 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
