

Associations between end-of-life discussion characteristics and care received near death: a prospective cohort study
- PMID: 23150700
- PMCID: PMC3675701
- DOI: 10.1200/JCO.2012.43.6055
Associations between end-of-life discussion characteristics and care received near death: a prospective cohort study
Abstract
Purpose: National guidelines recommend that discussions about end-of-life (EOL) care planning happen early for patients with incurable cancer. We do not know whether earlier EOL discussions lead to less aggressive care near death. We sought to evaluate the extent to which EOL discussion characteristics, such as timing, involved providers, and location, are associated with the aggressiveness of care received near death.
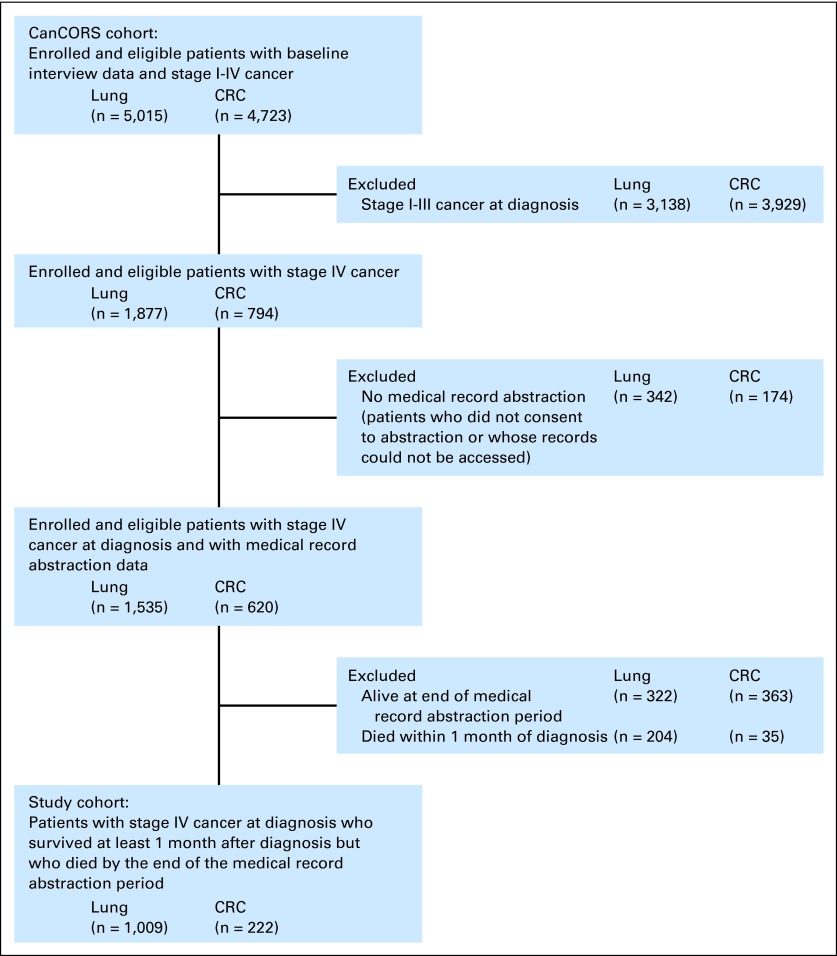
Patients and methods: We studied 1,231 patients with stage IV lung or colorectal cancer in the Cancer Care Outcomes Research and Surveillance Consortium, a population- and health system-based prospective cohort study, who died during the 15-month study period but survived at least 1 month. Our main outcome measure was the aggressiveness of EOL care received.
Results: Nearly half of patients received at least one marker of aggressive EOL care, including chemotherapy in the last 14 days of life (16%), intensive care unit care in the last 30 days of life (9%), and acute hospital-based care in the last 30 days of life (40%). Patients who had EOL discussions with their physicians before the last 30 days of life were less likely to receive aggressive measures at EOL, including chemotherapy (P = .003), acute care (P < .001), or any aggressive care (P < .001). Such patients were also more likely to receive hospice care (P < .001) and to have hospice initiated earlier (P < .001).
Conclusion: Early EOL discussions are prospectively associated with less aggressive care and greater use of hospice at EOL.
Figures
References
-
- Earle CC, Neville BA, Landrum MB, et al. Trends in the aggressiveness of cancer care near the end of life. J Clin Oncol. 2004;22:315–321. - PubMed
-
- Weeks JC, Cook EF, O'Day SJ, et al. Relationship between cancer patients' predictions of prognosis and their treatment preferences. JAMA. 1998;279:1709–1714. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
