

Trends in survival after in-hospital cardiac arrest
- PMID: 23150959
- PMCID: PMC3517894
- DOI: 10.1056/NEJMoa1109148
Trends in survival after in-hospital cardiac arrest
Abstract
Background: Despite advances in resuscitation care in recent years, it is not clear whether survival and neurologic function after in-hospital cardiac arrest have improved over time.
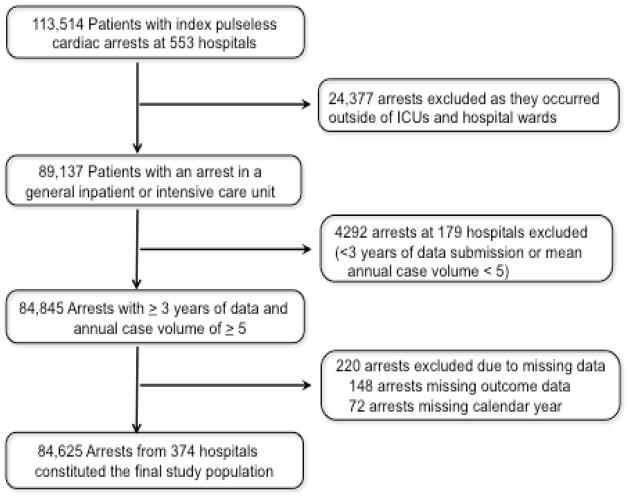
Methods: We identified all adults who had an in-hospital cardiac arrest at 374 hospitals in the Get with the Guidelines-Resuscitation registry between 2000 and 2009. Using multivariable regression, we examined temporal trends in risk-adjusted rates of survival to discharge. Additional analyses explored whether trends were due to improved survival during acute resuscitation or postresuscitation care and whether they occurred at the expense of greater neurologic disability in survivors.
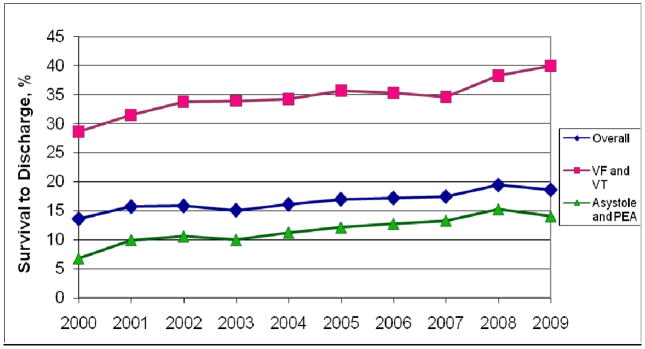
Results: Among 84,625 hospitalized patients with cardiac arrest, 79.3% had an initial rhythm of asystole or pulseless electrical activity, and 20.7% had ventricular fibrillation or pulseless ventricular tachycardia. The proportion of cardiac arrests due to asystole or pulseless electrical activity increased over time (P<0.001 for trend). Risk-adjusted rates of survival to discharge increased from 13.7% in 2000 to 22.3% in 2009 (adjusted rate ratio per year, 1.04; 95% confidence interval [CI], 1.03 to 1.06; P<0.001 for trend). Survival improvement was similar in the two rhythm groups and was due to improvement in both acute resuscitation survival and postresuscitation survival. Rates of clinically significant neurologic disability among survivors decreased over time, with a risk-adjusted rate of 32.9% in 2000 and 28.1% in 2009 (adjusted rate ratio per year, 0.98; 95% CI, 0.97 to 1.00; P=0.02 for trend).
Conclusions: Both survival and neurologic outcomes after in-hospital cardiac arrest have improved during the past decade at hospitals participating in a large national quality-improvement registry. (Funded by the American Heart Association.).
Figures
Comment in
-
Cardiac resuscitation. Increased survival for patients after in-hospital cardiac arrest.Nat Rev Cardiol. 2013 Jan;10(1):6. doi: 10.1038/nrcardio.2012.180. Epub 2012 Dec 4. Nat Rev Cardiol. 2013. PMID: 23207733 No abstract available.
-
Trends in survival after in-hospital cardiac arrest.N Engl J Med. 2013 Feb 14;368(7):680-1. doi: 10.1056/NEJMc1215155. N Engl J Med. 2013. PMID: 23406039 No abstract available.
-
Trends in survival after in-hospital cardiac arrest.N Engl J Med. 2013 Feb 14;368(7):680. doi: 10.1056/NEJMc1215155. N Engl J Med. 2013. PMID: 23406040 No abstract available.
References
-
- Rea TD, Crouthamel M, Eisenberg MS, Becker LJ, Lima AR. Temporal patterns in long-term survival after resuscitation from out-of-hospital cardiac arrest. Circulation. 2003;108:1196–201. - PubMed
-
- Hinchey PR, Myers JB, Lewis R, et al. Improved out-of-hospital cardiac arrest survival after the sequential implementation of 2005 AHA guidelines for compressions, ventilations, and induced hypothermia: the Wake County experience. Ann Emerg Med. 2003;56:348–57. - PubMed
-
- Pell JP, Corstorphine M, McConnachie A, et al. Post-discharge survival following pre-hospital cardiopulmonary arrest due to cardiac aetiology: temporal trends and impact of changes in clinical management. Eur Heart J. 2006;27:406–12. - PubMed
-
- Aufderheide TP, Yannopoulos D, Lick CJ, et al. Implementing the 2005 American Heart Association Guidelines improves outcomes after out-of-hospital cardiac arrest. Heart Rhythm. 2010;7:1357–62. - PubMed
-
- Hunt EA, Walker AR, Shaffner DH, Miller MR, Pronovost PJ. Simulation of in-hospital pediatric medical emergencies and cardiopulmonary arrests: highlighting the importance of the first 5 minutes. Pediatrics. 2008;121:e34–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous