

doi: 10.1016/j.clinimag.2012.02.016.
Epub 2012 Jun 8.
MRI perfusion in determining pseudoprogression in patients with glioblastoma
Affiliations
- PMID: 23151413
- PMCID: PMC4755513
- DOI: 10.1016/j.clinimag.2012.02.016
Item in Clipboard
MRI perfusion in determining pseudoprogression in patients with glioblastoma
Clin Imaging.
2013 Jan-Feb.
Abstract
We examine the role of dynamic susceptibility contrast (DSC) magnetic resonance imaging (MRI) perfusion in differentiating pseudoprogression from progression in 20 consecutive patients with treated glioblastoma. MRI perfusion was performed, and relative cerebral blood volume (rCBV), relative peak height (rPH), and percent signal recovery (PSR) were measured. Pseudoprogression demonstrated lower median rCBV (P=.009) and rPH (P<.001), and higher PSR (P=.039) than progression. DSC MRI perfusion successfully identified pseudoprogression in patients who did not require a change in treatment despite radiographic worsening following chemoradiotherapy.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
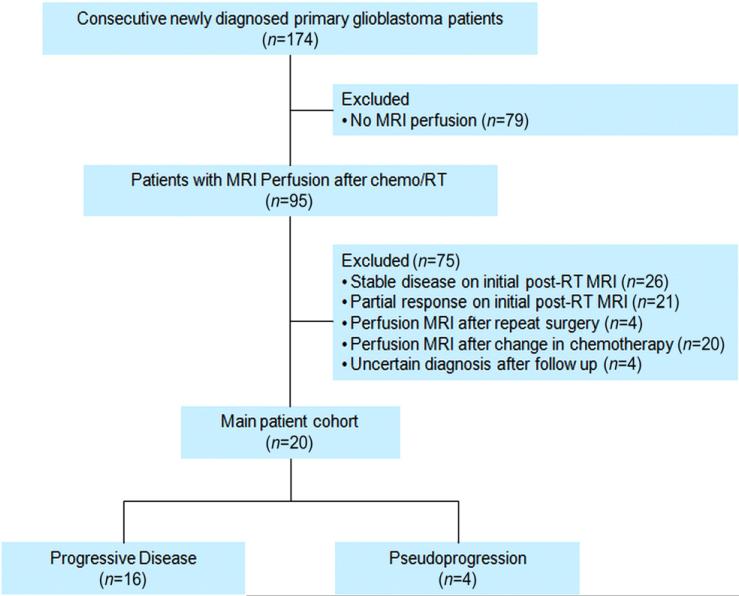
STARD diagram.

Distribution of rCBV in pseudoprogression and progressive disease.

Patient with pseudoprogression: (A–C) contrast axial T1-weighted images. One day (A) after gross total resection, there is a blood-filled surgical cavity in the lateral posterior frontal lobe without enhancement. One month after completion of RT (not shown), there is a new enhancing mass lesion that increases at 5 months (B) before decreasing at 12 months without a change in treatment (C). rCBV map (D) at 5 months does not show hyperperfusion of the enhancing lesion (ROI2) when compared to the contralateral normal white matter (ROI1). T2* signal intensity time curve (E) with rCBV, rPH, and PSR measurements.

Patient with progressive disease: (A–C) contrast axial T1-weighted images. (A) One day after gross total resection, there is a blood-filled surgical cavity in the parietal lobe with minor peripheral enhancement. (B) One month after completion of RT, a new enhancing mass lesion is seen at the treated site that nearly triples in size in (C) at 2 months. (D) rCBV map at 2 months shows moderate heterogeneous hyperperfusion of the enhancing lesion (ROI2) compared to the contralateral normal-appearing white matter (ROI1). T2* signal intensity time curve (E) with rCBV, rPH, and PSR measurements.
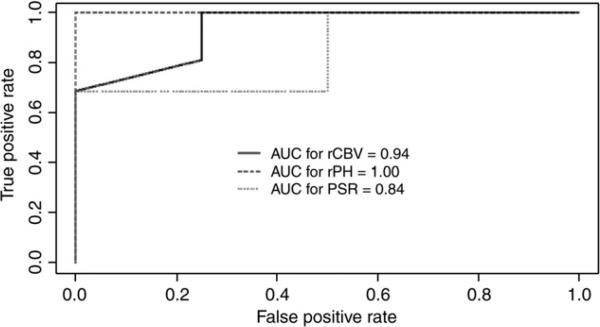
ROC analysis to detect progression using the following thresholds: rCBV≥1.80, rPH≥1.72, and PSR≤0.86.
References
-
- Macdonald DR, Cascino TL, Schold SC, Cairncross JG. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol. 1990;8(7):1277–80. - PubMed
-
- Brandsma D, Stalpers L, Taal W, Sminia P, van den Bent MJ. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol. 2008;9(5):453–61. - PubMed
-
- Chamberlain MC, Glantz MJ, Chalmers L, Van Horn A, Sloan AE. Early necrosis following concurrent Temodar and radiotherapy in patients with glioblastoma. J Neurooncol. 2007;82(1):81–3. - PubMed
-
- Brandes AA, Franceschi E, Tosoni A, et al. MGMT promoter methylation status can predict the incidence and outcome of pseudoprogression after concomitant radiochemotherapy in newly diagnosed glioblastoma patients. J Clin Oncol. 2008;26(13):2192–7. - PubMed
-
- Chaskis C, Neyns B, Michotte A, De Ridder M, Everaert H. Pseudoprogression after radiotherapy with concurrent temozolomide for high-grade glioma: clinical observations and working recommendations. Surg Neurol. 2009;72(4):423–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
