

Continuous and interrupted suturing techniques for repair of episiotomy or second-degree tears
- PMID: 23152204
- PMCID: PMC7045987
- DOI: 10.1002/14651858.CD000947.pub3
Continuous and interrupted suturing techniques for repair of episiotomy or second-degree tears
Abstract
Background: Millions of women worldwide undergo perineal suturing after childbirth and the type of repair may have an impact on pain and healing. For more than 70 years, researchers have been suggesting that continuous non-locking suture techniques for repair of the vagina, perineal muscles and skin are associated with less perineal pain than traditional interrupted methods.
Objectives: To assess the effects of continuous versus interrupted absorbable sutures for repair of episiotomy and second-degree perineal tears following childbirth.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (20 January 2012).
Selection criteria: Randomised trials examining continuous and interrupted suturing techniques for repair of episiotomy and second-degree tears after vaginal delivery.
Data collection and analysis: Three review authors independently assessed trial quality. Two of the three authors independently extracted data and a third review author checked them. We contacted study authors for additional information.
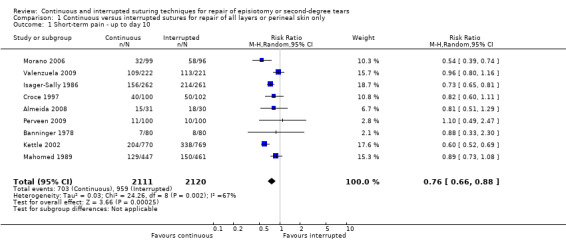
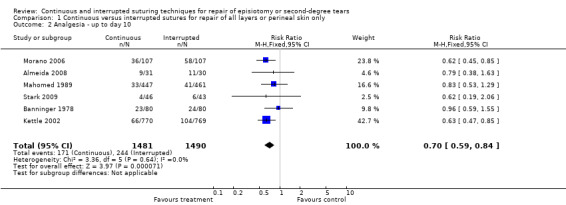
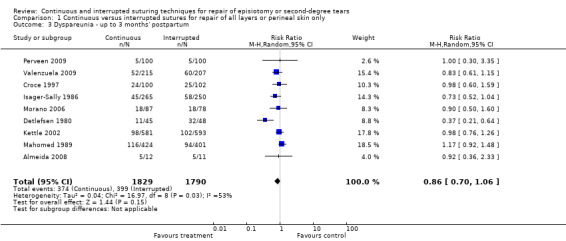
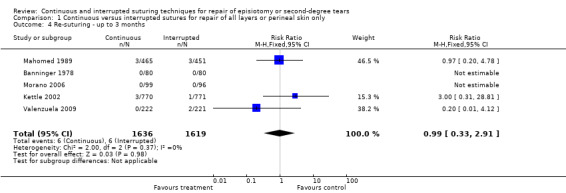
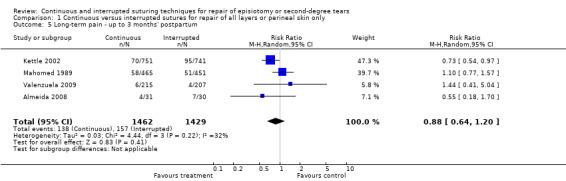
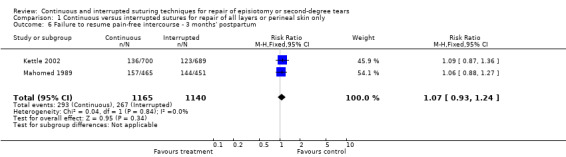
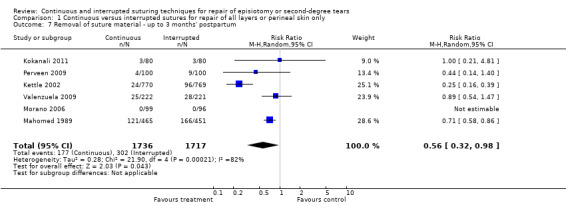
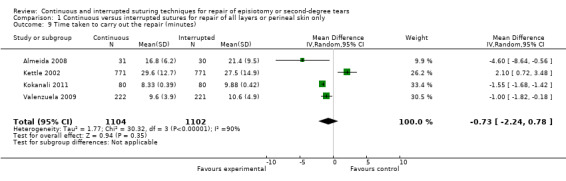
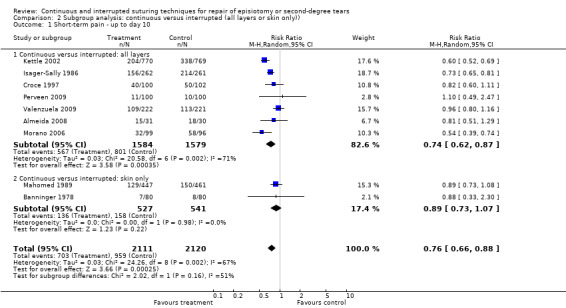
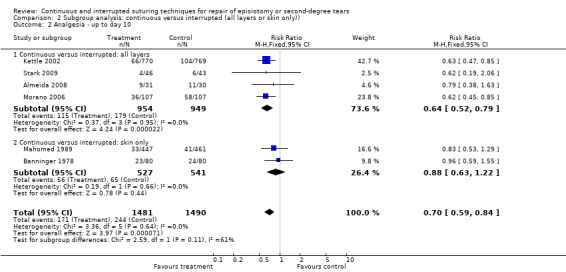
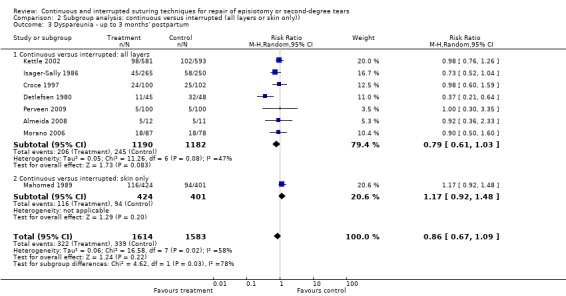
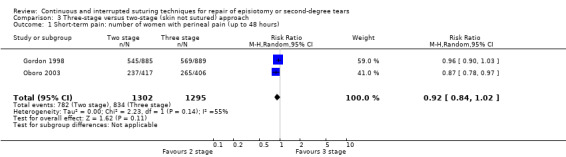
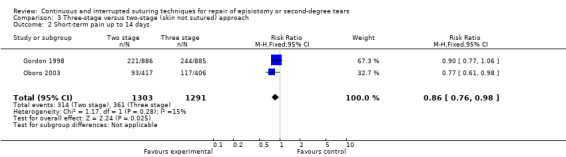
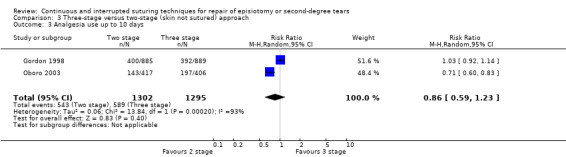
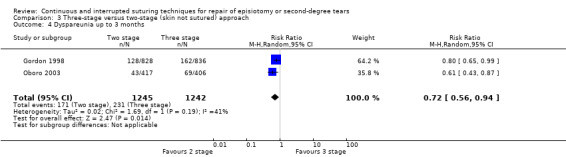
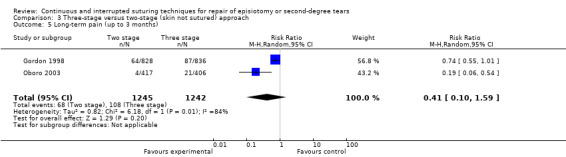
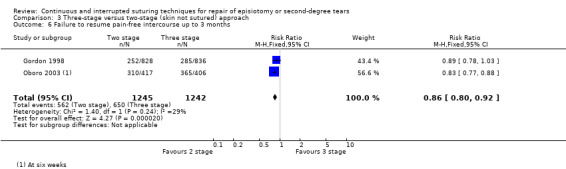
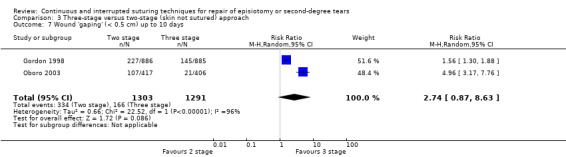
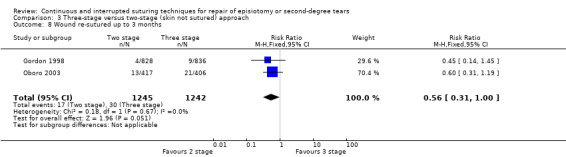
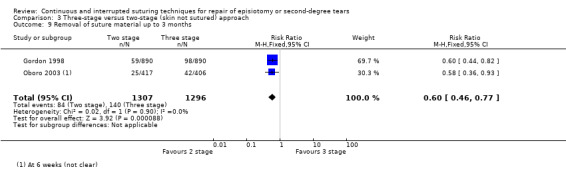
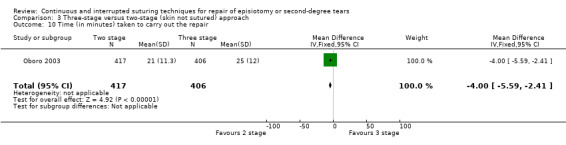
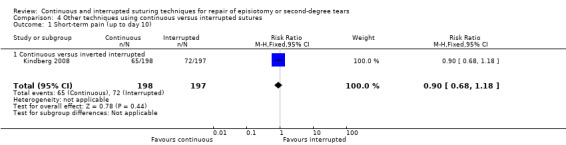
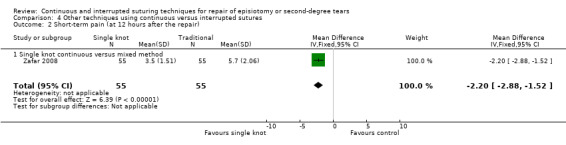
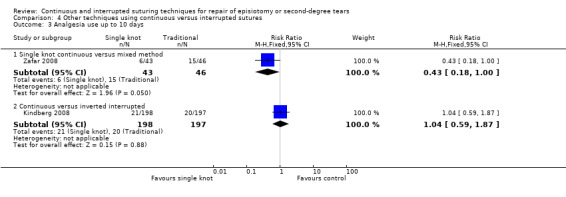
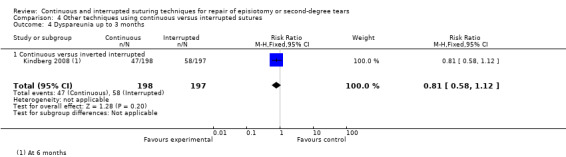
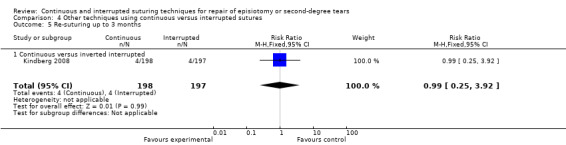
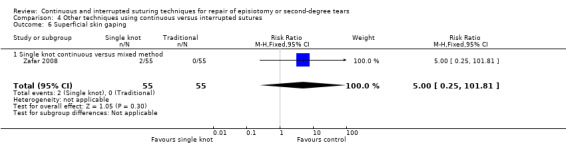
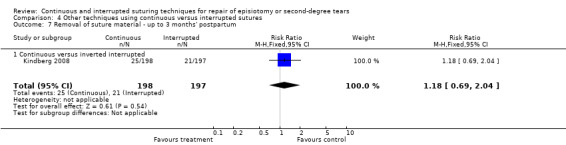
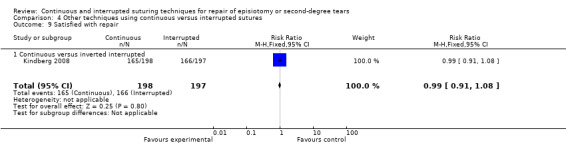
Main results: Sixteen studies, involving 8184 women at point of entry, from eight countries, were included. The trials were heterogeneous in respect of operator skill and training. Meta-analysis showed that continuous suture techniques compared with interrupted sutures for perineal closure (all layers or perineal skin only) are associated with less pain for up to 10 days' postpartum (risk ratio (RR) 0.76; 95% confidence interval (CI) 0.66 to 0.88, nine trials). There was an overall reduction in analgesia use associated with the continuous subcutaneous technique versus interrupted stitches for repair of perineal skin (RR 0.70; 95% CI 0.59 to 0.84). There was also a reduction in suture removal in the continuous suturing groups versus interrupted (RR 0.56; 95% CI 0.32 to 0.98), but no significant differences were seen in the need for re-suturing of wounds or long-term pain.
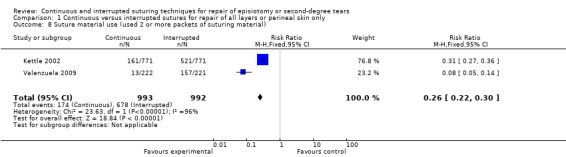
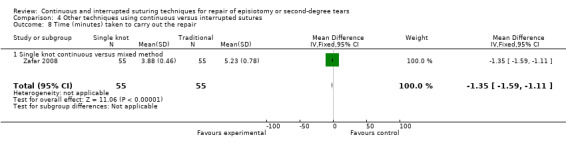
Authors' conclusions: The continuous suturing techniques for perineal closure, compared with interrupted methods, are associated with less short-term pain, need for analgesia and suture removal. Furthermore, there is also some evidence that the continuous techniques used less suture material as compared with the interrupted methods (one packet compared to two or three packets, respectively).
Conflict of interest statement
Christine Kettle (CK) was the recipient of a fellowship from the Iolanthe Midwifery Research Trust 1996, which provided funding to enable her to carry out a randomised controlled trial of perineal repair following childbirth (Kettle 2002). The Iolanthe Midwifery Research Trust and Ethicon Ltd, UK (manufacturers of suture material) provided funding for employment of a part‐time data management clerk for that trial.
CK and Khaled Ismail run perineal repair workshops both nationally and internationally and have developed an episiotomy and second‐degree tear training model with Limbs & Things, UK.
Figures
Update of
-
Continuous versus interrupted sutures for repair of episiotomy or second degree tears.Cochrane Database Syst Rev. 2007 Oct 17;(4):CD000947. doi: 10.1002/14651858.CD000947.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2012 Nov 14;11:CD000947. doi: 10.1002/14651858.CD000947.pub3. PMID: 17943747 Updated.
References
References to studies included in this review
Almeida 2008 {published data only}
-
- Almeida SF, Riesco ML. Randomized controlled clinical trial on two perineal trauma suture techniques in normal delivery. Revista Latino‐Americana de Enfermagem 2008;16(2):272‐9. - PubMed
Banninger 1978 {published data only}
-
- Banninger U, Buhrig H, Schreiner WE. A comparison between chromic catgut and polyglycolic acid sutures in episiotomy repair. Geburtshilfe und Frauenheilkunde 1978;38:30‐3. - PubMed
Croce 1997 {published data only}
-
- Croce P, Signorelli P, Dede A, Galli D. Selective episiotomy. Comparison of two suture techniques. Minerva Ginecologica 1997;49:449‐53. - PubMed
Detlefsen 1980 {published data only}
-
- Detlefsen GU, Vinther S, Larsen P, Schroeder E. Intradermal suturing of episiotomy wounds compared with interrupted sutures. Ugeskrift for Laeger 1980;142:3117‐20. - PubMed
Gordon 1998 {published data only}
-
- D'Souza D. The Ipswich Childbirth Study: 1 A randomised evaluation of two stage postpartum perineal repair leaving the skin unsutured [letter; comment]. British Journal of Obstetrics and Gynaecology 1999;106(1):89‐90. - PubMed
-
- Gordon B, Mackrodt C, Fern E, Truesdale A, Ayers S, Grant A. The Ipswich Childbirth Study: 1. A randomised evaluation of two stage postpartum perineal repair leaving the skin unsutured. British Journal of Obstetrics and Gynaecology 1998;105:435‐40. - PubMed
-
- Grant A, Gordon B, Mackrodt C, Fern E, Truesdale A, Ayers S. The Ipswich Childbirth Study: one year follow up of alternative methods used in perineal repair. BJOG: an International Journal of Obstetrics and Gynaecology 2001;108(1):34‐40. - PubMed
-
- Mackrodt C, Fern E, Gordon B. Ipswich Childbirth Study ‐ perineal suturing study. Proceedings of Research in Midwifery Conference; 1993 Sept 14; Birmingham, UK. 1993.
Isager‐Sally 1986 {published data only}
-
- Isager‐Sally I, Legarth J, Jacobsen B, Bostofte E. Episiotomy repair ‐ immediate and long‐term sequelae. A prospective randomized study of three different methods of repair. British Journal of Obstetrics and Gynaecology 1986;93:420‐5. - PubMed
Kettle 2002 {published data only}
-
- Kettle C, Hills R, Jones P, Darby L, Gray R, Johanson R. Continuous versus interrupted perineal repair with standard or rapidly absorbed sutures after spontaneous vaginal birth: a randomised controlled trial. Lancet 2002;359:2217‐23. - PubMed
Kindberg 2008 {published data only}
-
- Kindberg S, Stehouwer M, Hvidman L, Henriksen TB. Postpartum perineal repair performed by midwives: a randomised trial comparing two suture techniques leaving the skin unsutured. BJOG: an International Journal of Obstetrics and Gynaecology 2008;115(4):472‐9. - PubMed
Kokanali 2011 {published data only}
-
- Kokanali D, Ugur M, Kuntay M, Karayalcin R, Tonguc E. Continuous versus interrupted episiotomy repair with monofilament or multifilament absorbed suture materials: a randomised controlled trial. Archives of Gynecology and Obstetrics 2011;284(2):275‐80. - PubMed
Mahomed 1989 {published data only}
-
- Mahomed K, Grant AM, Ashurst H, James D. The Southmead perineal suture study. A randomized comparison of suture materials and suturing techniques for repair of perineal trauma. British Journal of Obstetrics and Gynaecology 1989;96:1272‐80. - PubMed
Morano 2006 {published data only}
-
- Morano S, Mistrangelo E, Pastorino D, Lijoi D, Costantini S, Ragni N. A randomized comparison of suturing techniques for episiotomy and laceration repair after spontaneous vaginal birth. Journal of Minimally Invasive Gynecology 2006;13(5):457‐62. - PubMed
Oboro 2003 {published data only}
-
- Oboro VO, Tabowei TO, Bosah JO. A multicentre evaluation of the two‐layered repair of postpartum perineal trauma. Journal of Obstetrics and Gynaecology 2003;23(1):5‐8. - PubMed
Perveen 2009 {published data only}
-
- Perveen F, Shabbir T. Perineal repair: comparison of suture materials and suturing techniques. Journal of Surgery Pakistan 2009;14(1):23‐8.
Stark 2009 {published data only}
-
- Stark M. Episiotomy ‐ the destructive tradition. Gineco.ro 2009;5(3):142‐5.
Valenzuela 2009 {published data only}
-
- Valenzuela P, Saiz Puente MS, Valero JL, Azorin R, Ortega R, Guijarro R. Continuous versus interrupted sutures for repair of episiotomy or second‐degree perineal tears: a randomised controlled trial. BJOG: an International Journal of Obstetrics and Gynaecology 2009;116(3):436‐41. - PubMed
Zafar 2008 {published data only}
-
- Zafar S. Comparison of a single‐knot versus three layered technique of perineal repair after vaginal delivery in women requiring episiotomy: a double blind randomized controlled trial. Journal of the Turkish‐German Gynecology Association 2008;9(3):129‐33.
References to studies excluded from this review
Bendsen 1980 {published data only}
-
- Bendsen J, Madsen H. Intracutaneous suturing of episiotomy wounds. Comparison between polyglycolic acid (Dexon) intracutaneously and silk sutures in the skin. Ugeskrift for Laeger 1980;142:3120‐2. - PubMed
Buchan 1980 {published data only}
Doyle 1993 {published data only}
-
- Doyle PM, Johanson R, Geetha T, Wilkinson P. A prospective randomised controlled trial of perineal repair after childbirth, comparing interrupted chromic catgut to subcuticular prolene for skin closure. British Journal of Obstetrics and Gynaecology 1993;100:93‐4. - PubMed
Hansen 1975 {published data only}
-
- Hansen MK, Selnes A, Simonsen E, Sorensen KM, Pedersen GT. Polyglycolic acid (Dexon) used as suture material for the repair of episiotomies. Ugeskrift for Laeger 1975;137:617‐20. - PubMed
Roberts 1993 {published data only}
-
- Roberts M, Richardson L, Johnson D, Coleman S, Michael EM. A randomised trial of perineal repair following childbirth: a comparison of subcuticular polyglactin 910 (Vicryl) and interrupted black silk for perineal skin closure. Online Journal of Current Clinical Trials 1993;2:Doc 90.
References to studies awaiting assessment
Graczyk 1998 {published data only}
-
- Graczyk S, Limanowski M, Wyduba M. Interrupted vs. subcuticular technique of episiotomy wound repair in clinical and cosmetic aspects. Ginekologia Polska 1998;69(1):6‐11. - PubMed
Uslu 1992 {published data only}
-
- Uslu MA, Ozekici U, Simsek M, Berkman S. A prospective randomized study of three different methods of episiotomy repair. Istanbul Tip Fakultesi Mecumasi 1992;55:237‐42.
Additional references
Fernando 2006
Glazener 1995
-
- Glazener CMA, Abdalla M, Stroud P, Naji S, Templeton A, Russell IT. Postnatal maternal morbidity: extent, causes, prevention and treatment. British Journal of Obstetrics and Gynaecology 1995;102:286‐7. - PubMed
Greenland 1987
-
- Greenland S. Quantitative methods in the review of epidemiologic literature. Epidemiologic Reviews 1987;9:1‐30. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Kettle 2010
Klein 1994
-
- Klein MC, Gauthier RJ, Robbins JM, Kaczorowski J, Jorgensen SH, Franco ED, et al. Relationship of episiotomy to perineal trauma and morbidity, sexual dysfunction, and pelvic floor relaxation. American Journal of Obstetrics and Gynecology 1994;171:591‐8. - PubMed
McCandlish 1998
-
- McCandlish R, Bowler U, Asten H, Berridge G, Winter C, Sames L, et al. A randomised controlled trial of care of the perineum during second stage of normal labour. British Journal of Obstetrics and Gynaecology 1998;105(12):1262‐72. - PubMed
RevMan 2011 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
Sleep 1984
Sleep 1991
-
- Sleep J. Perineal care: a series of five randomised controlled trials. In: Robinson S, Thompson A editor(s). Midwives, Research and Childbirth. Vol. 2, London: Chapman and Hall, 1991.
References to other published versions of this review
Johanson 1995
-
- Johanson RB. Continuous vs interrupted sutures for perineal repair [revised 10th March 1994]. In: Enkin MW, Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C (eds.) Pregnancy and Childbirth Module. In: The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM]. The Cochrane Collaboration; Issue 2, Oxford: Update Software. 1995.