

Early hematopoietic stem cell transplant is associated with favorable outcomes in children with MDS
- PMID: 23152304
- PMCID: PMC3668778
- DOI: 10.1002/pbc.24390
Early hematopoietic stem cell transplant is associated with favorable outcomes in children with MDS
Abstract
Background: Although hematopoietic stem cell transplantation (HSCT) is the treatment of choice for childhood myelodysplastic syndrome (MDS), there is no consensus regarding patient or disease characteristics that predict outcomes.
Procedure: We reviewed 37 consecutive pediatric MDS patients who received myeloablative HSCT between 1990 and 2010 at a single center.
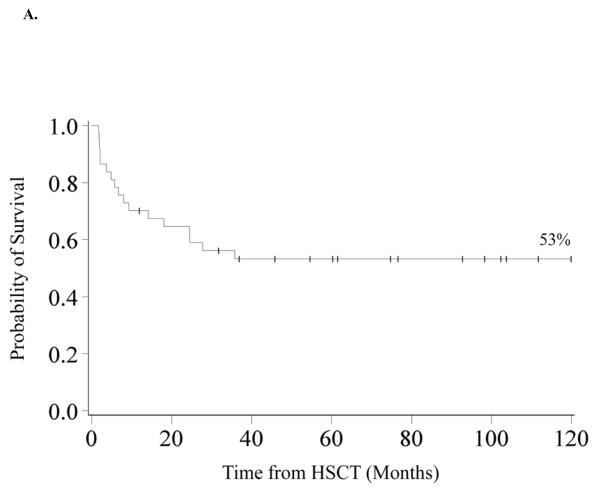
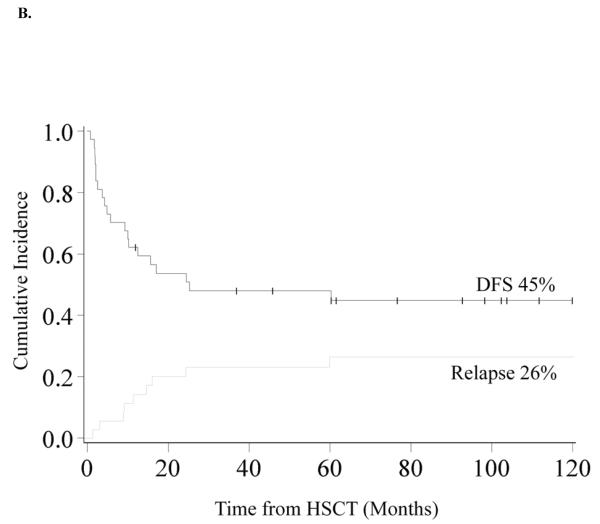
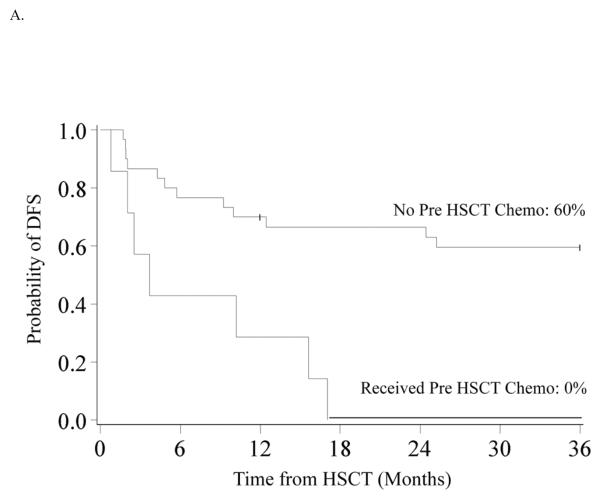
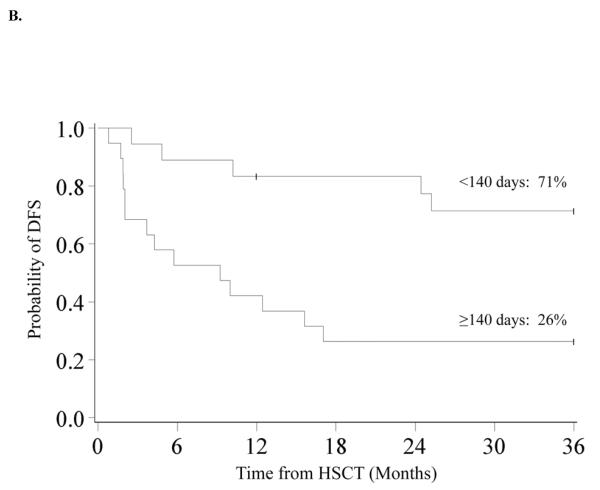
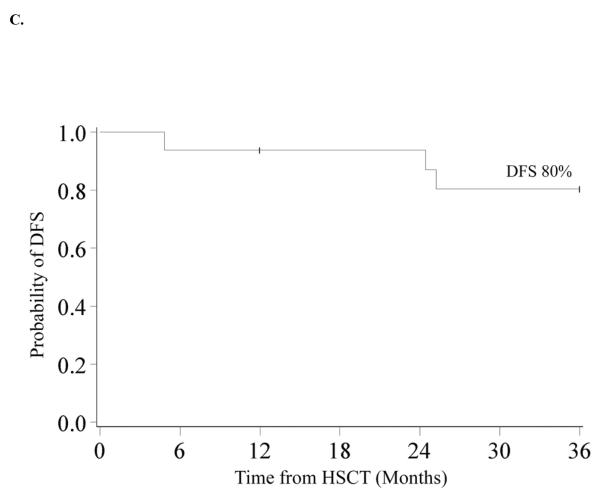
Results: Twenty had primary MDS and 17 had secondary MDS. Diagnostic cytogenetics included monosomy 7 (n = 21), trisomy 8 (n = 7) or normal/other (n = 8). According to the modified WHO MDS classification, thirty had refractory cytopenia and seven had refractory anemia with excess blasts. IPSS scores were: low risk (n = 1), intermediate-1 (n = 15), and intermediate-2 (n = 21). OS and DFS at 10 years in the entire cohort was 53% and 45%. Relapse at 10 years was 26% and 1 year TRM was 25%. In multivariate analysis, factors associated with improved 3 years DFS were not receiving pre-HSCT chemotherapy (RR = 0.30, 95% CI 0.10-0.88; P = 0.03) and a shorter interval (<140 days) from time of diagnosis to transplant (RR = 0.27, 95% CI 0.09-0.80; P = 0.02). Three years DFS in patients who did not receive pre-HSCT chemotherapy and those who had a shorter interval to transplant (n = 16) was 80%.
Conclusion: These results suggest that children with MDS should be referred for allogeneic HSCT soon after diagnosis and that pre-HSCT chemotherapy does not appear to improve outcomes.
Copyright © 2012 Wiley Periodicals, Inc.
Figures
Similar articles
-
Improving Revised International Prognostic Scoring System Pre-Allogeneic Stem Cell Transplantation Does Not Translate Into Better Post-Transplantation Outcomes for Patients with Myelodysplastic Syndromes: A Single-Center Experience.Biol Blood Marrow Transplant. 2018 Jun;24(6):1209-1215. doi: 10.1016/j.bbmt.2018.02.007. Epub 2018 Feb 20. Biol Blood Marrow Transplant. 2018. PMID: 29474870
-
Allogeneic stem cell transplantation for adults with myelodysplastic syndromes: importance of pretransplant disease burden.Biol Blood Marrow Transplant. 2009 Jan;15(1):30-8. doi: 10.1016/j.bbmt.2008.10.012. Biol Blood Marrow Transplant. 2009. PMID: 19135940
-
Allogeneic hematopoietic stem cell transplantation for pediatric patients with treatment-related myelodysplastic syndrome or acute myelogenous leukemia.Biol Blood Marrow Transplant. 2012 Mar;18(3):473-80. doi: 10.1016/j.bbmt.2011.11.009. Epub 2011 Nov 10. Biol Blood Marrow Transplant. 2012. PMID: 22079789
-
[Hematopoietic stem cell transplantation in the myelodisplastic syndromes].Rev Invest Clin. 2005 Mar-Apr;57(2):283-90. Rev Invest Clin. 2005. PMID: 16524069 Review. Spanish.
-
Advances in the prognostication and management of advanced MDS in children.Br J Haematol. 2011 Jul;154(2):185-95. doi: 10.1111/j.1365-2141.2011.08724.x. Epub 2011 May 9. Br J Haematol. 2011. PMID: 21554264 Review.
Cited by
-
[Clinical analysis of the therapeutic effect of allogeneic hematopoietic stem cell transplantation in 10 cases of childhood myelodysplastic syndrome/myeloproliferative neoplasm].Zhonghua Xue Ye Xue Za Zhi. 2018 Feb 14;39(2):162-164. doi: 10.3760/cma.j.issn.0253-2727.2018.02.018. Zhonghua Xue Ye Xue Za Zhi. 2018. PMID: 29562455 Free PMC article. Chinese. No abstract available.
-
Disease Burden at the Time of Transplantation Is a Primary Predictor of Outcomes in Pediatric MDS: A Single-Center Experience.Cancers (Basel). 2025 May 13;17(10):1645. doi: 10.3390/cancers17101645. Cancers (Basel). 2025. PMID: 40427141 Free PMC article.
-
Thrombocytopenia in MDS: epidemiology, mechanisms, clinical consequences and novel therapeutic strategies.Leukemia. 2016 Mar;30(3):536-44. doi: 10.1038/leu.2015.297. Epub 2015 Oct 26. Leukemia. 2016. PMID: 26500138 Review.
-
A Rare Concurrence of Myelodysplastic Neoplasia and Tetrasomy 8 in a 3-Year-Old Bahraini Male.Cureus. 2023 Jul 17;15(7):e41988. doi: 10.7759/cureus.41988. eCollection 2023 Jul. Cureus. 2023. PMID: 37593262 Free PMC article.
-
A familial SAMD9 variant present in pediatric myelodysplastic syndrome.Cold Spring Harb Mol Case Stud. 2023 May 9;9(2):a006256. doi: 10.1101/mcs.a006256. Print 2023 Apr. Cold Spring Harb Mol Case Stud. 2023. PMID: 37160314 Free PMC article.
References
-
- Smith FO, Woods WG. Myeloproliferative and myelodysplastic disorders. In: Pizzo PA, Poplack DG, editors. Principles and practice of pediatric oncology. Lippincott Williams & Wilkins; Philadelphia: 2002. p. 615.
-
- Niemeyer C, Baumann I. Myelodysplastic syndrome in children and adolescents. Semin.Hematol. 2008;45:60–70. - PubMed
-
- Hasle H, Niemeyer CM, Chessells JM, et al. A pediatric approach to the WHO classification of myelodysplastic and myeloproliferative diseases. Leukemia. 2003;17:277–282. - PubMed
-
- Hasle H. Myelodysplastic and myeloproliferative disorders in children. Curr Opin Pediatr. 2007;19:1–8. - PubMed
-
- Locatelli F, Zecca M, Pession A, Maserati E, De Stefano P, Severi F. Myelodysplastic syndromes: the pediatric point of view. Haematologica. 1995;80:268–279. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
