

Randomized, placebo-controlled trial of mipomersen in patients with severe hypercholesterolemia receiving maximally tolerated lipid-lowering therapy
- PMID: 23152839
- PMCID: PMC3496741
- DOI: 10.1371/journal.pone.0049006
Randomized, placebo-controlled trial of mipomersen in patients with severe hypercholesterolemia receiving maximally tolerated lipid-lowering therapy
Abstract
Objectives: Mipomersen, an antisense oligonucleotide targeting apolipoprotein B synthesis, significantly reduces LDL-C and other atherogenic lipoproteins in familial hypercholesterolemia when added to ongoing maximally tolerated lipid-lowering therapy. Safety and efficacy of mipomersen in patients with severe hypercholesterolemia was evaluated.
Methods and results: Randomized, double-blind, placebo-controlled, multicenter trial. Patients (n = 58) were ≥18 years with LDL-C ≥7.8 mmol/L or LDL-C ≥5.1 mmol/L plus CHD disease, on maximally tolerated lipid-lowering therapy that excluded apheresis. Weekly subcutaneous injections of mipomersen 200 mg (n = 39) or placebo (n = 19) were added to lipid-lowering therapy for 26 weeks.
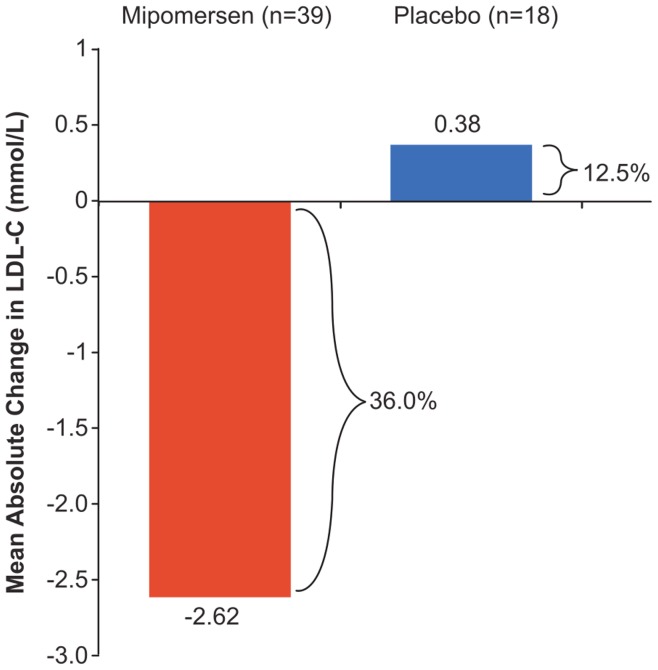
Main outcome: percent reduction in LDL-C from baseline to 2 weeks after the last dose of treatment. Mipomersen (n = 27) reduced LDL-C by 36%, from a baseline of 7.2 mmol/L, for a mean absolute reduction of 2.6 mmol/L. Conversely, mean LDL-C increased 13% in placebo (n = 18) from a baseline of 6.5 mmol/L (mipomersen vs placebo p<0.001). Mipomersen produced statistically significant (p<0.001) reductions in apolipoprotein B and lipoprotein(a), with no change in high-density lipoprotein cholesterol. Mild-to-moderate injection site reactions were the most frequently reported adverse events with mipomersen. Mild-to-moderate flu-like symptoms were reported more often with mipomersen. Alanine transaminase increase, aspartate transaminase increase, and hepatic steatosis occurred in 21%, 13% and 13% of mipomersen treated patients, respectively. Adverse events by category for the placebo and mipomersen groups respectively were: total adverse events, 16(84.2%), 39(100%); serious adverse events, 0(0%), 6(15.4%); discontinuations due to adverse events, 1(5.3%), 8(20.5%) and cardiac adverse events, 1(5.3%), 5(12.8%).
Conclusion: Mipomersen significantly reduced LDL-C, apolipoprotein B, total cholesterol and non-HDL-cholesterol, and lipoprotein(a). Mounting evidence suggests it may be a potential pharmacologic option for lowering LDL-C in patients with severe hypercholesterolemia not adequately controlled using existing therapies. Future studies will explore alternative dosing schedules aimed at minimizing side effects.
Trial registration: ClinicalTrials.gov NCT00794664.
Conflict of interest statement
Figures


References
-
- National Lipid Association Expert panel on Familial Hypercholesterolemia (2011) Familial hypercholesterolemias: Prevalence, genetics, diagnosis and screening recommendations from the National Lipid Association Expert panel on Familial Hypercholesterolemia. J Clin Lipidol 5: S9–S17. - PubMed
-
- Civeira F, for the International Panel on Management of Familial Hypercholesterolemia (2004) Guidelines for the diagnosis and management of heterozygous familial hypercholesterolemia. Atherosclerosis 173(1): 55–68. - PubMed
-
- Avis HJ, Visser MN, Stein EA, Wijburg FA, Trip MD, et al. (2007) A systematic review and meta-analysis of statin therapy in children with familial hypercholesterolemia. Arterioscler Thromb Vasc Biol 27(8): 1803–1810. - PubMed
-
- Rodenburg J, Vissers MN, Wiegman A, van Trotsenburg AS, van der Graaf A, et al. (2007) Statin treatment in children with familial hypercholesterolemia: the younger, the better. Circulation 116(6): 664–668. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
