

IgG responses to Pneumococcal and Haemophilus influenzae protein antigens are not impaired in children with a history of recurrent acute otitis media
- PMID: 23152850
- PMCID: PMC3495775
- DOI: 10.1371/journal.pone.0049061
IgG responses to Pneumococcal and Haemophilus influenzae protein antigens are not impaired in children with a history of recurrent acute otitis media
Abstract
Background: Vaccines including conserved antigens from Streptococcus pneumoniae and nontypeable Haemophilus influenzae (NTHi) have the potential to reduce the burden of acute otitis media. Little is known about the antibody response to such antigens in young children with recurrent acute otitis media, however, it has been suggested antibody production may be impaired in these children.
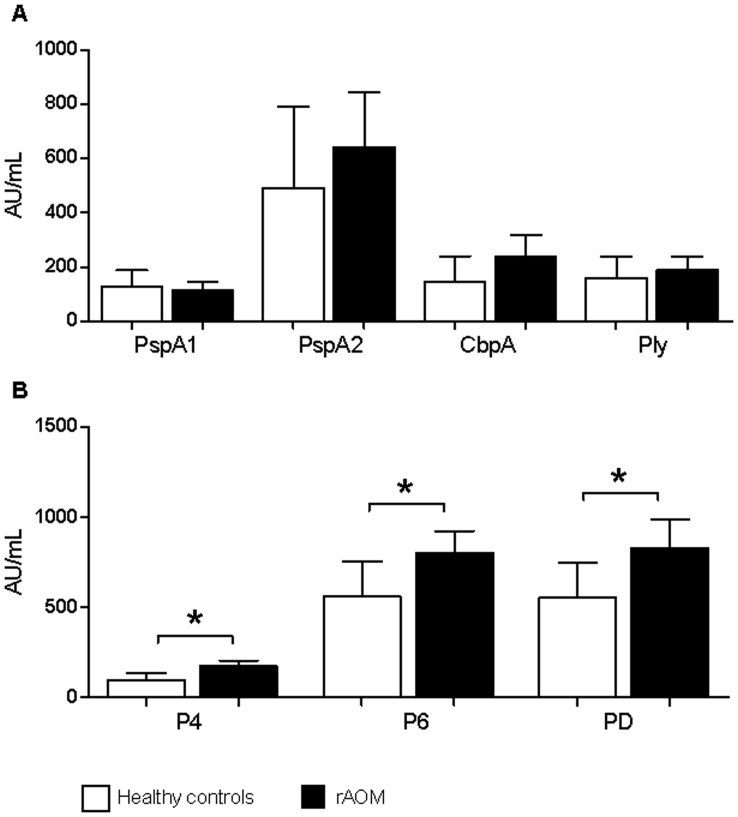
Methods: We measured serum IgG levels against 4 pneumococcal (PspA1, PspA 2, CbpA and Ply) and 3 NTHi (P4, P6 and PD) proteins in a cross-sectional study of 172 children under 3 years of age with a history of recurrent acute otitis media (median 7 episodes, requiring ventilation tube insertion) and 63 healthy age-matched controls, using a newly developed multiplex bead assay.
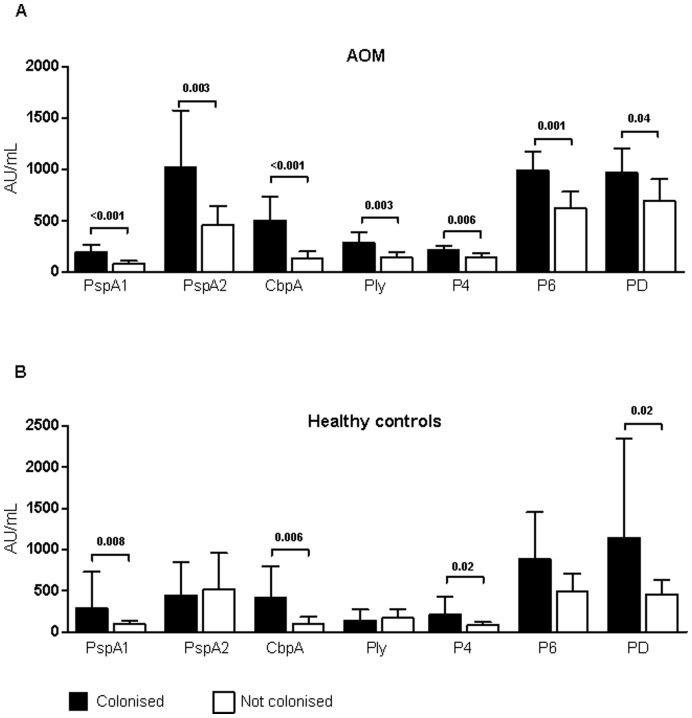
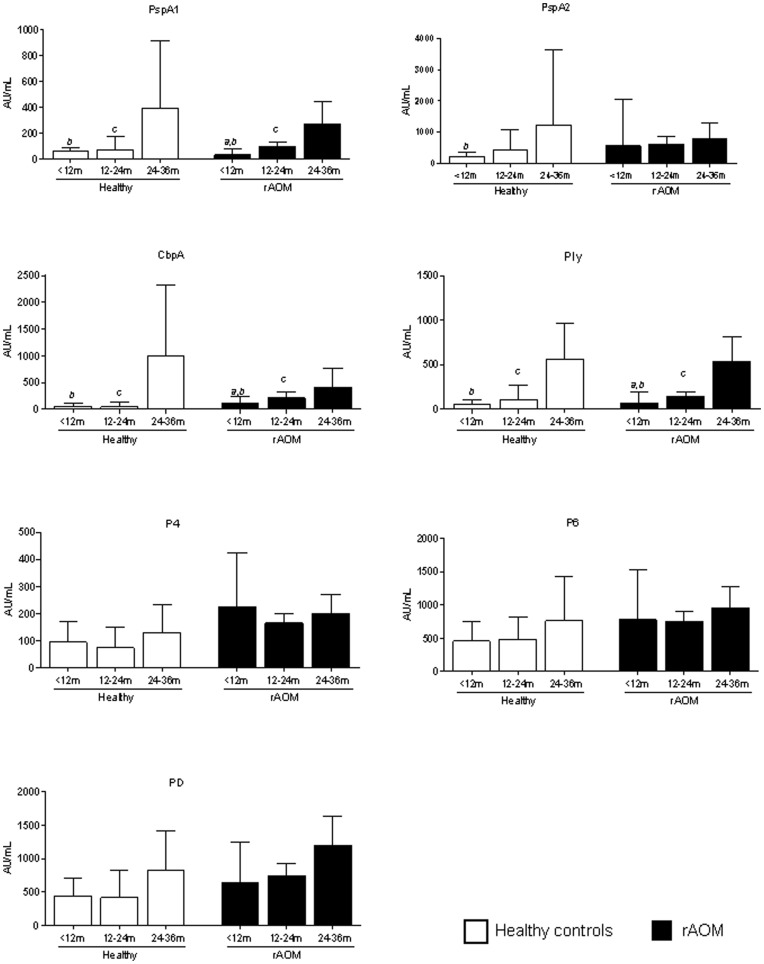
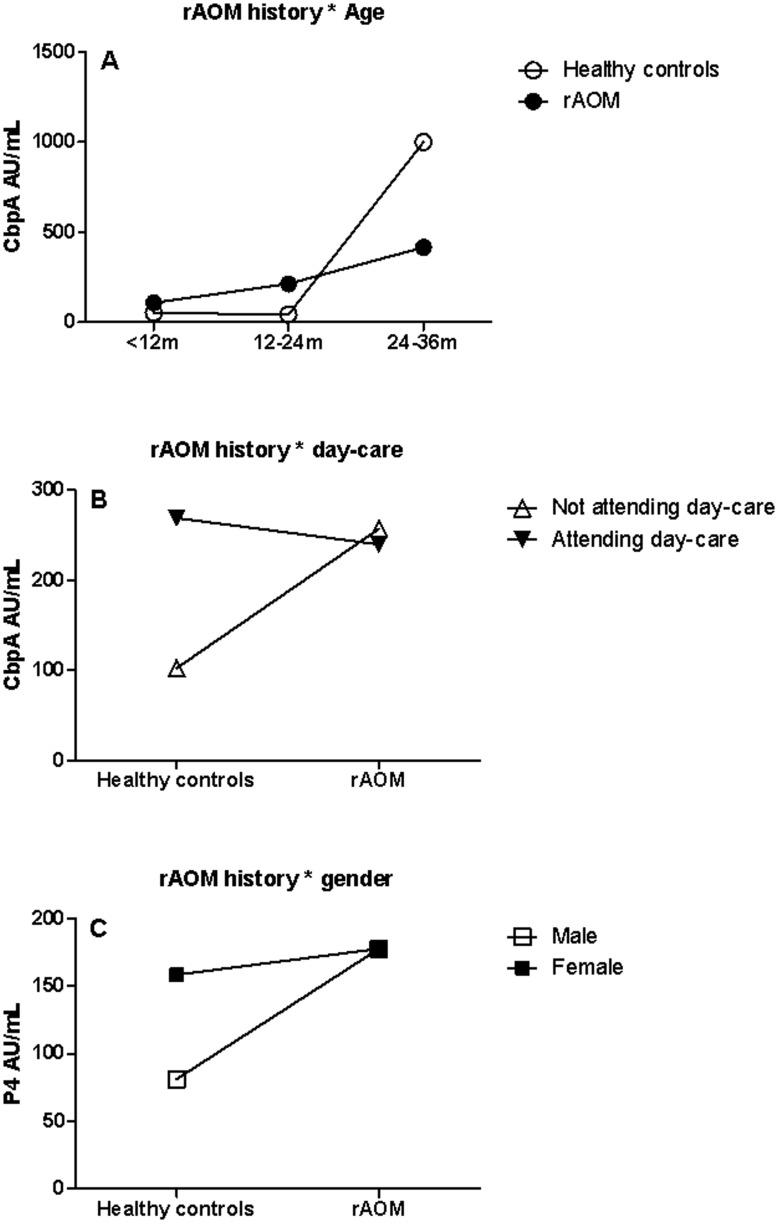
Results: Children with a history of recurrent acute otitis media had significantly higher geometric mean serum IgG levels against NTHi proteins P4, P6 and PD compared with healthy controls, whereas there was no difference in antibody levels against pneumococcal protein antigens. In both children with and without a history of acute otitis media, antibody levels increased with age and were significantly higher in children colonised with S. pneumoniae or NTHi compared with children that were not colonised.
Conclusions: Proteins from S. pneumoniae and NTHi induce serum IgG in children with a history of acute otitis media. The mechanisms in which proteins induce immunity and potential protection requires further investigation but the dogma of impaired antibody responses in children with recurrent acute otitis media should be reconsidered.
Conflict of interest statement
Figures
References
-
- Vergison A, Dagan R, Arguedas A, Bonhoeffer J, Cohen R, et al. (2010) Otitis media and its consequences: beyond the earache. Lancet Infect Dis 10: 195–203. - PubMed
-
- Pletz MW, Maus U, Krug N, Welte T, Lode H (2008) Pneumococcal vaccines: mechanism of action, impact on epidemiology and adaption of the species. Int J Antimicrob Agents 32: 199–206. - PubMed
-
- Block SL, Hedrick J, Harrison CJ, Tyler R, Smith A, et al. (2004) Community-wide vaccination with the heptavalent pneumococcal conjugate significantly alters the microbiology of acute otitis media. PediatrInfectDisJ 23: 829. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
