

Sarcoidosis and chronic hepatitis C: a case report
- PMID: 23155326
- PMCID: PMC3484354
- DOI: 10.3748/wjg.v18.i40.5816
Sarcoidosis and chronic hepatitis C: a case report
Abstract
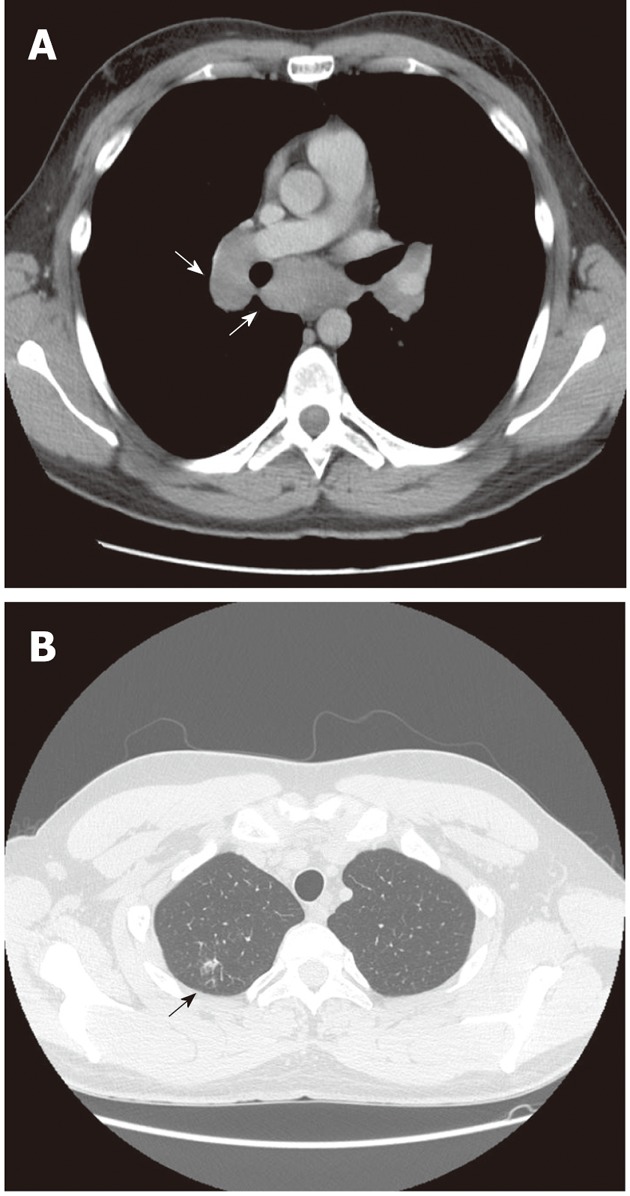
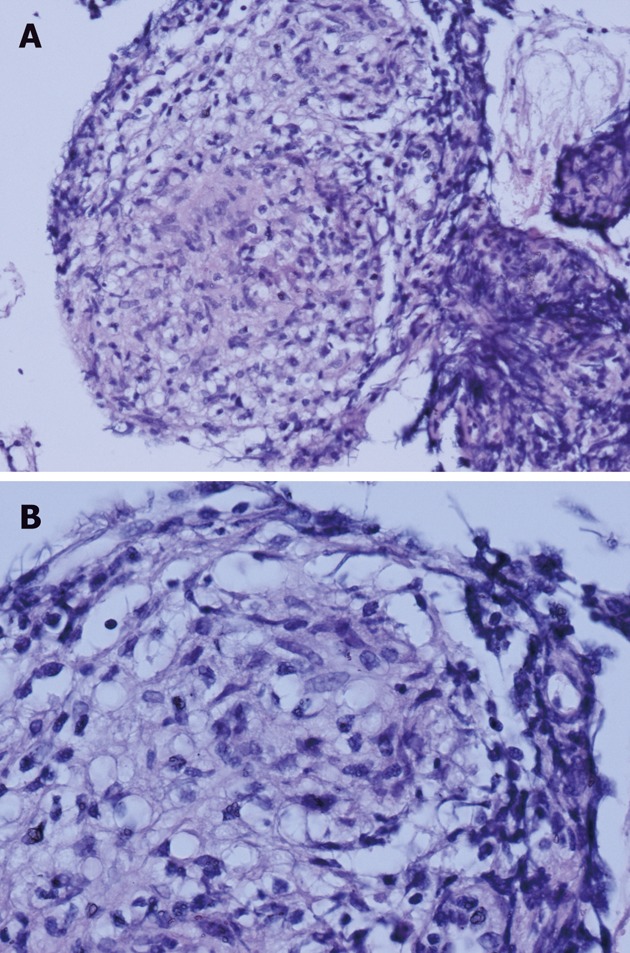
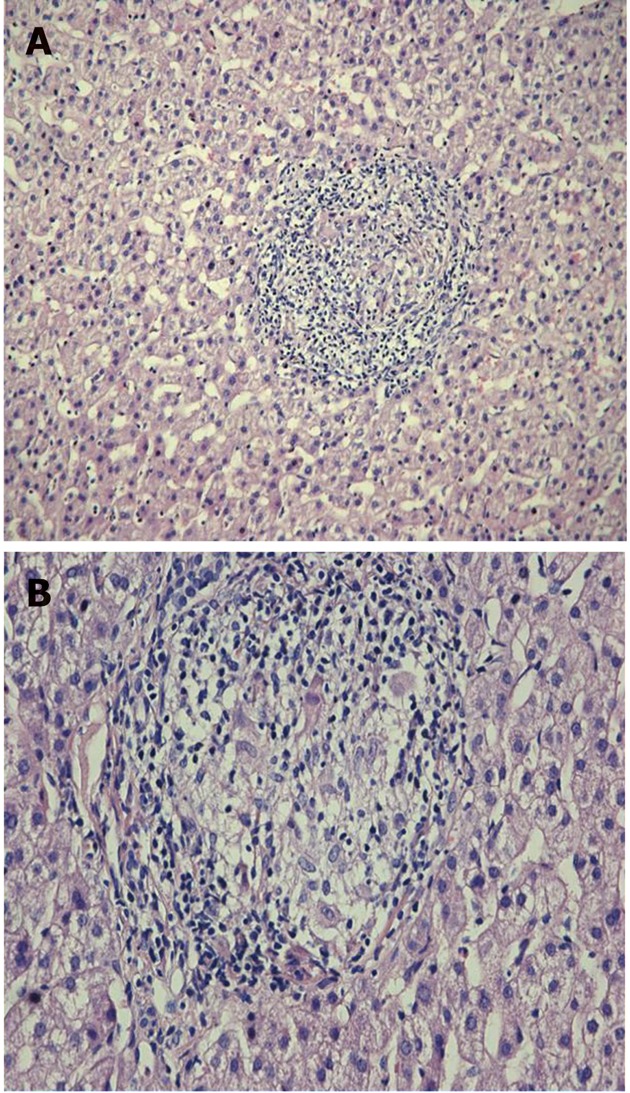
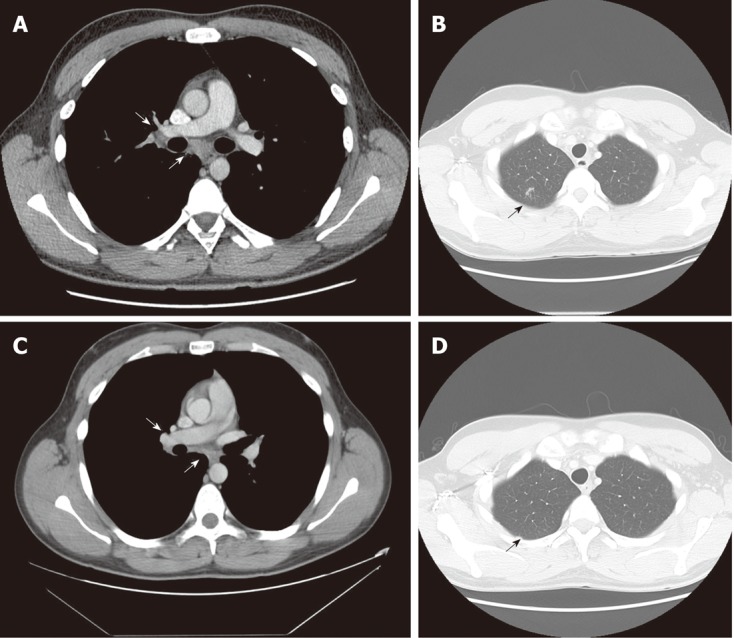
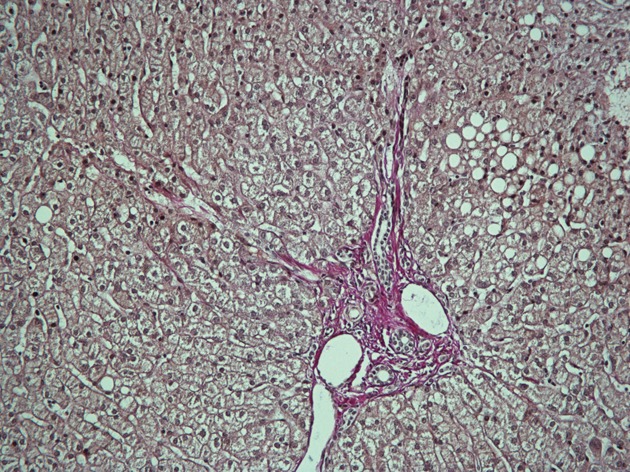
Several case reports deal with the relationship between hepatitis C virus (HCV) infection and pulmonary or hepatic sarcoidosis. Most publications describe interferon α-induced sarcoidosis. However, HCV infection per se is also suggested to cause sarcoidosis. The present case report describes a case of biopsy-verified lung and liver sarcoidosis and HCV infection, and the outcome of antiviral therapy. In March 2009, a 25-year-old man presented with moderately elevated liver enzymes without any clinical symptoms. The patient was positive for HCV antibodies and HCV RNA of genotype 1b. Four months later the patient became dyspnoic and pulmonary sarcoidosis was diagnosed by lung biopsy and radiography. A short course of corticosteroid treatment relieved symptoms. Three months later, liver biopsy showed noncaseating granulomas consisting of epithelioid histiocytes and giant cells with a small amount of peripheral lymphocyte infiltration, without any signs of fibrosis. Chronic HCV infection with coexistence of pulmonary and hepatic sarcoidosis was diagnosed. Antiviral therapy with peginterferon α and ribavirin at standard doses was started, which lasted 48 wk, and sustained viral response was achieved. A second liver biopsy showed disappearance of granulomas and chest radiography revealed normalization of mediastinal and perihilar glands. The hypothesis that HCV infection per se may have triggered systemic sarcoidosis was proposed. Successful treatment of HCV infection led to continuous remission of pulmonary and hepatic sarcoidosis. Further studies are required to understand the relationship between systemic sarcoidosis and HCV infection.
Keywords: Hepatitis C virus infection; Peginterferon α; Pulmonary and hepatic sarcoidosis; Ribavirin; Sustained viral response.
Figures
References
-
- Baldo V, Baldovin T, Trivello R, Floreani A. Epidemiology of HCV infection. Curr Pharm Des. 2008;14:1646–1654. - PubMed
-
- Tefanova V, Tallo T, Kutsar K, Priimgi L. Urgent action needed to stop spread of hepatitis B and C in Estonian drug users. Euro Surveill. 2006;11:E060126.3. - PubMed
-
- Agnello V, De Rosa FG. Extrahepatic disease manifestations of HCV infection: some current issues. J Hepatol. 2004;40:341–352. - PubMed
-
- Zignego AL, Ferri C, Pileri SA, Caini P, Bianchi FB. Extrahepatic manifestations of Hepatitis C Virus infection: a general overview and guidelines for a clinical approach. Dig Liver Dis. 2007;39:2–17. - PubMed
-
- Costabel U, Hunninghake GW. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders. Eur Respir J. 1999;14:735–737. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
