

Outcomes after listing with a requirement for a prospective crossmatch in pediatric heart transplantation
- PMID: 23157944
- PMCID: PMC3603363
- DOI: 10.1016/j.healun.2012.09.023
Outcomes after listing with a requirement for a prospective crossmatch in pediatric heart transplantation
Abstract
Background: Allosensitization is associated with inferior waitlist outcomes in pediatric heart transplant candidates, presumably because of the requirement for a negative prospective crossmatch. However, there are no reports of heart transplant candidate outcomes according to prospective crossmatch requirements.
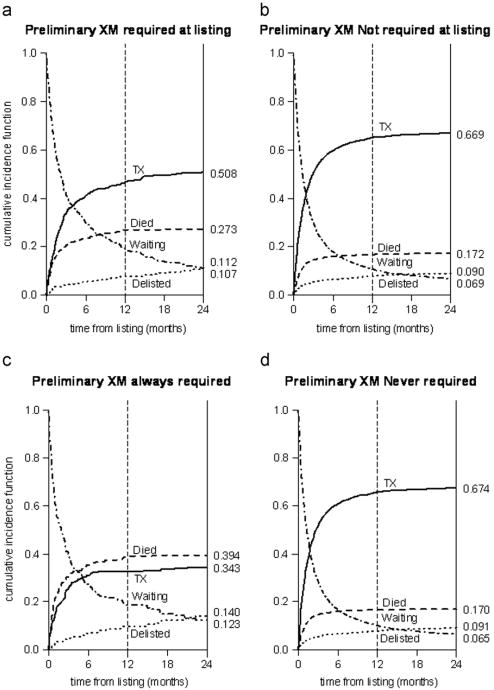
Methods: We analyzed data on all children listed for isolated heart transplantation from 1995 to 2009 in the USA according to prospective crossmatch requirement (PXMR). Primary objectives were to describe the prevalence of PXMR at and during listing and to compare waitlist and post-transplant survival for patients based on PXMR. Patients with a PXMR during listing include those with a PXMR at the time of listing as well as those who were designated by the listing center as needing a prospective crossmatch at some point after being placed onto the waitlist.
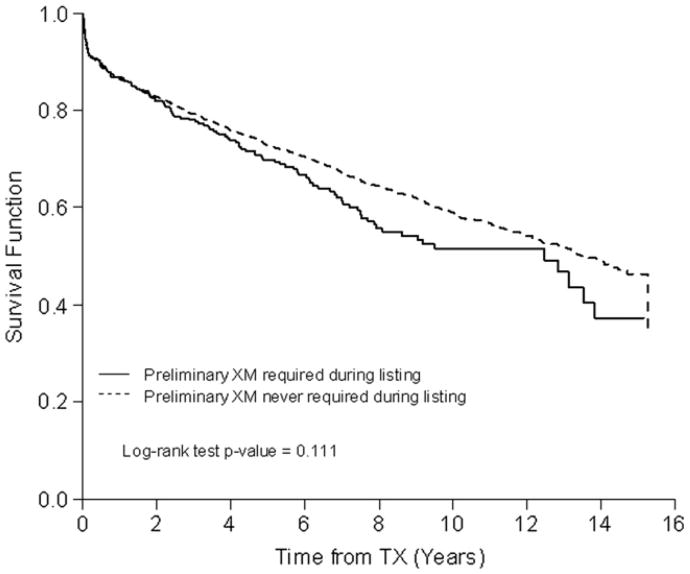
Results: Among 6,343 listed children, 7.7% had a requirement for a prospective crossmatch at the time of listing and 11.8% had a requirement for a prospective crossmatch during listing. After controlling for risk factors associated with inferior survival, PXMR at listing was associated with increased waitlist mortality (HR 1.32, 95% CI 1.10 to 1.56; p = 0.003). Recipients with a PXMR during listing more commonly had a positive DSXM (22.1% vs 10.3%, p < 0.0001), as did recipients who carried a PXMR throughout listing (21.7% vs 11.3%, p = 0.004). However, there was no significant difference in post-transplant survival on the basis of a PXMR during listing (HR 1.04, 95% CI 0.87 to 1.25; p = 0.67). Nearly 30% of recipients with a PXMR during listing had a peak pre-transplant PRA ≤ 10%.
Conclusions: PXMR increases the likelihood of death while awaiting, but not after, pediatric heart transplantation. Further study is necessary to understand how PXMR is applied, and changes, after listing for pediatric heart transplantation.
Copyright © 2013 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Feingold B, Bowman P, Zeevi A, et al. Survival in allosensitized children after listing for cardiac transplantation. J Heart Lung Transplant. 2007;26:565–71. - PubMed
-
- Mahle WT, Tresler MA, Edens RE, et al. Allosensitization and outcomes in pediatric heart transplantation. J Heart Lung Transplant. 2011;30:1221–7. - PubMed
-
- Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94:496–509.
-
- Dipchand AI, Naftel DC, Feingold B, et al. Outcomes of children with cardiomyopathy listed for transplant: a multi-institutional study. J Heart Lung Transplant. 2009;28:1312–21. - PubMed
-
- Jacobs JP, Quintessenza JA, Boucek RJ, et al. Pediatric cardiac transplantation in children with high panel reactive antibody. Ann Thorac Surg. 2004;78:1703–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
