

Out-of-pocket healthcare payments on chronic conditions impoverish urban poor in Bangalore, India
- PMID: 23158475
- PMCID: PMC3533578
- DOI: 10.1186/1471-2458-12-990
Out-of-pocket healthcare payments on chronic conditions impoverish urban poor in Bangalore, India
Abstract
Background: The burden of chronic conditions is on the rise in India, necessitating long-term support from healthcare services. Healthcare, in India, is primarily financed through out-of-pocket payments by households. Considering scarce evidence available from India, our study investigates whether and how out-of-pocket payments for outpatient care affect individuals with chronic conditions.
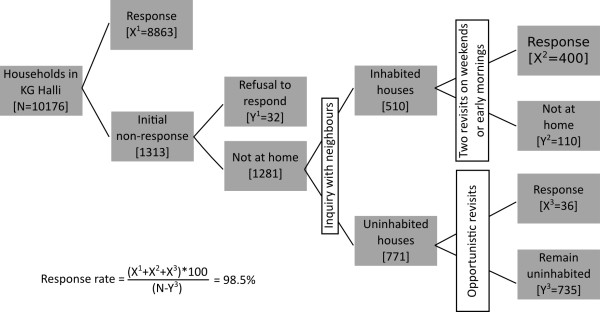
Methods: A large census covering 9299 households was conducted in Bangalore, India. Of these, 3202 households that reported presence of chronic condition were further analysed. Data was collected using a structured household-level questionnaire. Out-of-pocket payments, catastrophic healthcare expenditure, and the resultant impoverishment were measured using a standard technique.
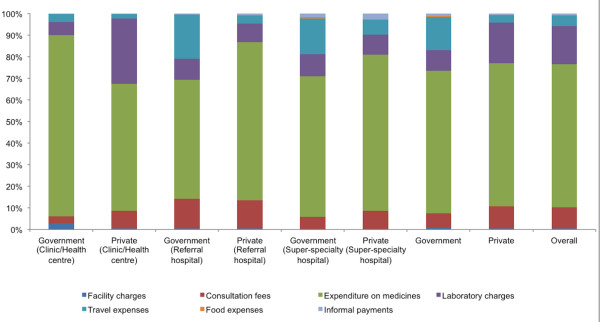
Results: The response rate for the census was 98.5%. Overall, 69.6% (95%CI=68.0-71.2) of households made out-of-pocket payments for outpatient care spending a median of 3.2% (95%CI=3.0-3.4) of their total income. Overall, 16% (95%CI=14.8-17.3) of households suffered financial catastrophe by spending more than 10% of household income on outpatient care. Occurrence and intensity of financial catastrophe were inequitably high among poor. Low household income, use of referral hospitals as place for consultation, and small household size were associated with a greater likelihood of incurring financial catastrophe.The out-of-pocket spending on chronic conditions doubled the number of people living below the poverty line in one month, with further deepening of their poverty. In order to cope, households borrowed money (4.2% instances), and sold or mortgaged their assets (0.4% instances).
Conclusions: This study provides evidence from India that the out-of-pocket payment for chronic conditions, even for outpatient care, pushes people into poverty. Our findings suggest that improving availability of affordable medications and diagnostics for chronic conditions, as well as strengthening the gate keeping function of the primary care services are important measures to enhance financial protection for urban poor. Our findings call for inclusion of outpatient care for chronic conditions in existing government-initiated health insurance schemes.
Figures
References
-
- Samb B, Desai N, Nishtar S, Mendis S, Bekedam H, Wright A, Hsu J, Martiniuk A, Celletti F, Patel K, Adshead F, McKee M, Evans T, Alwan A, Etienne C. Prevention and management of chronic disease: a litmus test for health-systems strengthening in low-income and middle-income countries. Lancet. 2010;376:1785–1797. doi: 10.1016/S0140-6736(10)61353-0. - DOI - PubMed
-
- World Health Organization. Everybody’s business: Strengthening health systems to improve health outcomes: WHO's framework for action. Geneva: WHO Press; 2007.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
