

Hemodialysis access usage patterns in the incident dialysis year and associated catheter-related complications
- PMID: 23159234
- PMCID: PMC3532948
- DOI: 10.1053/j.ajkd.2012.09.006
Hemodialysis access usage patterns in the incident dialysis year and associated catheter-related complications
Abstract
Background: Hemodialysis (HD) access is considered a critical and actionable determinant of morbidity, with a growing literature suggesting that initial HD access type is an important marker of long-term outcomes. Accordingly, we examined HD access during the incident dialysis period, focusing on infection risk and successful fistula creation during the first dialysis year.
Study design: Longitudinal cohort.
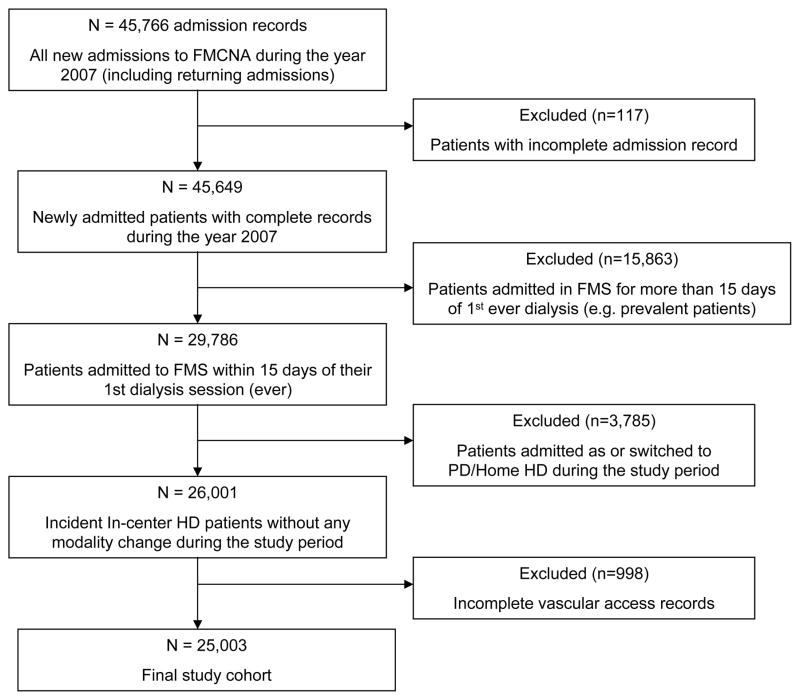
Setting & participants: All US adults admitted to Fresenius Medical Care North America facilities within 15 days of first maintenance dialysis session between January 1 and December 31, 2007.
Predictor: Vascular access type at HD therapy initiation.
Outcomes: Vascular access type at 90 days and at the end of the first year on HD therapy, bloodstream infection within the first year by access type, and catheter complication rate.
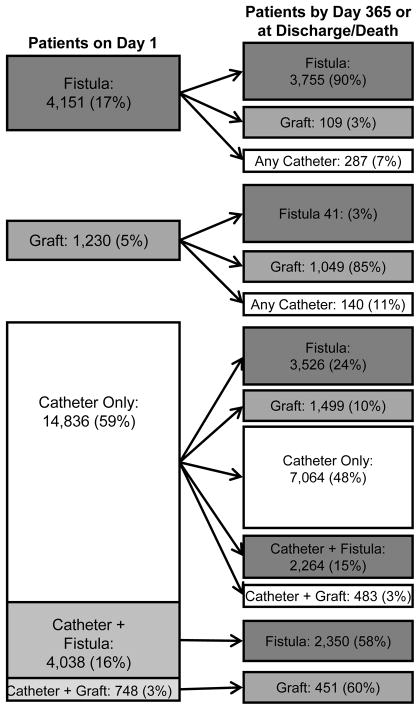
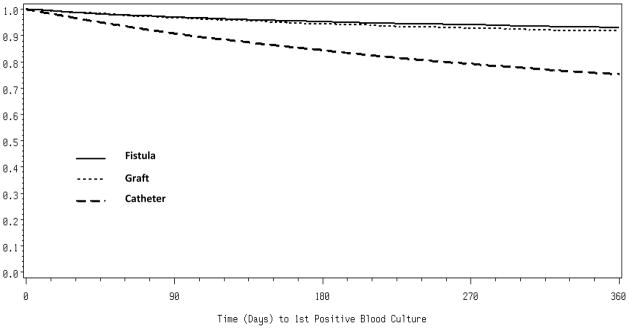
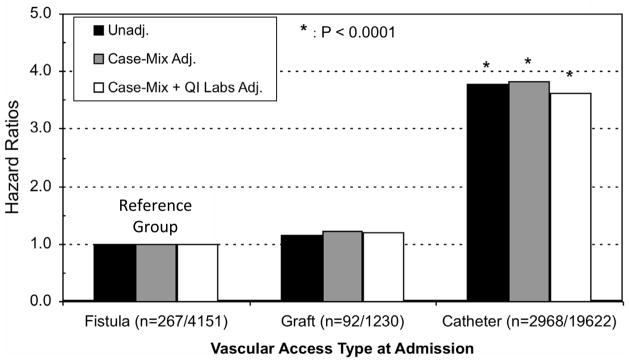
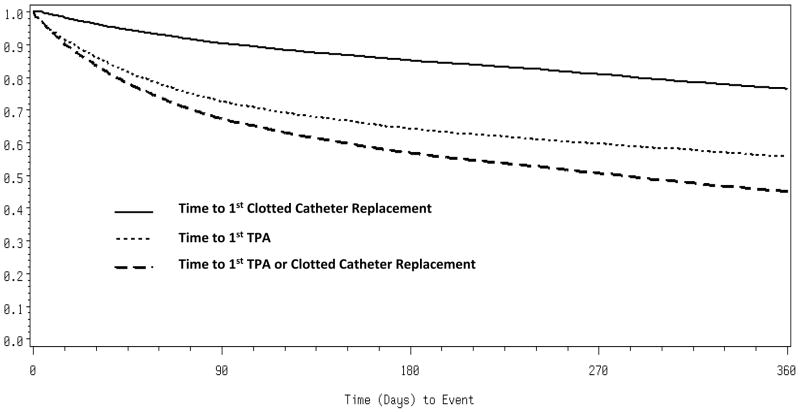
Results: Of 25,003 incident dialysis patients studied, 19,622 (78.5%) initiated dialysis with a catheter; 4,151 (16.6%), with a fistula; and 1,230 (4.9%), with a graft. At 90 days, 14,105 (69.7%) had a catheter, 4,432 (21.9%) had a fistula, and 1,705 (8.4%) had a graft. Functioning fistulas and grafts at dialysis therapy initiation had first-year failure rates of 10% and 15%, respectively. Grafts were seldom replaced by fistulas (3%), whereas 7,064 (47.6%) of all patients who initiated with a catheter alone still had only a catheter at 1 year. Overall, 3,327 (13.3%) patients had at least one positive blood culture during follow-up, with the risk being similar between the fistula and graft groups, but approximately 3-fold higher in patients with a catheter (P<0.001 for either comparison). Nearly 1 in 3 catheters (32.5%) will require tissue plasminogen activator use by a median of 41 days, with 59% requiring more than one tissue plasminogen activator administration.
Limitations: Potential underestimation of bacteremia because follow-up blood culture results did not include samples sent to local laboratories.
Conclusions: In a large and representative population of incident US dialysis patients, catheter use remains very high during the first year of HD care and is associated with high mechanical complication and bloodstream infection rates.
Copyright © 2012 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Thrombolytic protocol potentially reduces catheter-related complications in hemodialysis patients.Am J Kidney Dis. 2013 Sep;62(3):643. doi: 10.1053/j.ajkd.2013.04.027. Am J Kidney Dis. 2013. PMID: 23972061 No abstract available.
-
In reply to 'Thrombolytic protocol potentially reduces catheter-related complications in hemodialysis patients'.Am J Kidney Dis. 2013 Sep;62(3):643. doi: 10.1053/j.ajkd.2013.06.014. Am J Kidney Dis. 2013. PMID: 23972062 No abstract available.
References
-
- Bradbury BD, Fissell RB, Albert JM, Anthony MS, Critchlow CW, Pisoni RL, et al. Predictors of early mortality among incident US hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS) Clin J Am Soc Nephrol. 2007;2(1):89–99. - PubMed
-
- Astor BC, Eustace JA, Powe NR, Klag MJ, Fink NE, Coresh J. Type of vascular access and survival among incident hemodialysis patients: the Choices for Healthy Outcomes in Caring for ESRD (CHOICE) Study. J Am Soc Nephrol. 2005;16(5):1449–55. - PubMed
-
- Gulati S, Sahu KM, Avula S, Sharma RK, Ayyagiri A, Pandey CM. Role of vascular access as a risk factor for infections in hemodialysis. Ren Fail. 2003;25(6):967–73. - PubMed
-
- Powe NR, Jaar B, Furth SL, Hermann J, Briggs W. Septicemia in dialysis patients: incidence, risk factors, and prognosis. Kidney Int. 1999;55(3):1081–90. - PubMed
-
- Dhingra RK, Young EW, Hulbert-Shearon TE, Leavey SF, Port FK. Type of vascular access and mortality in U.S. hemodialysis patients. Kidney Int. 2001;60(4):1443–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
