

Anatomical basis and histopathological changes resulting from selective internal radiotherapy for liver metastases
- PMID: 23162108
- PMCID: PMC3595145
- DOI: 10.1136/jclinpath-2012-201231
Anatomical basis and histopathological changes resulting from selective internal radiotherapy for liver metastases
Abstract
Background: Knowledge that liver tumours preferentially take their blood supply from the arterial blood supply rather than the portal venous system can be used for local delivery of treatment or for embolisation to cut off the blood supply to tumours.
Aims: To present histological evaluation of malignant and non-malignant hepatic tissue of one such therapy, selective internal radiation therapy (SIRT) with yttrium-90 microspheres, to decipher its principal mechanism of action.
Methods: The H&E stained sections of hepatic resection specimens from three patients with liver metastases from colorectal (CRC) cancer, who underwent hepatic surgery 4-9 months following SIRT, were examined and the pathological changes documented.
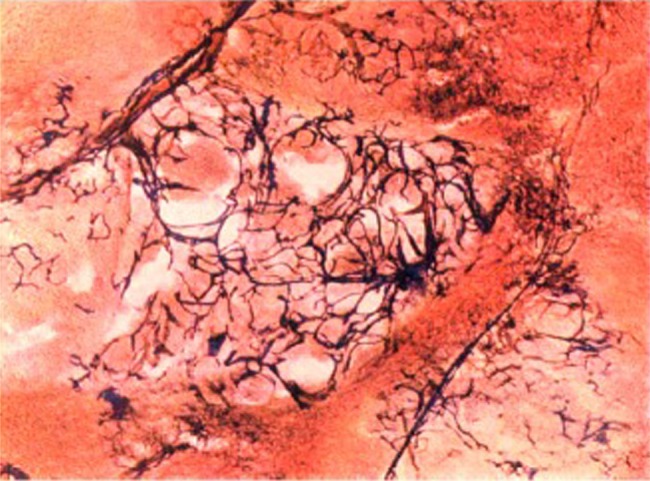
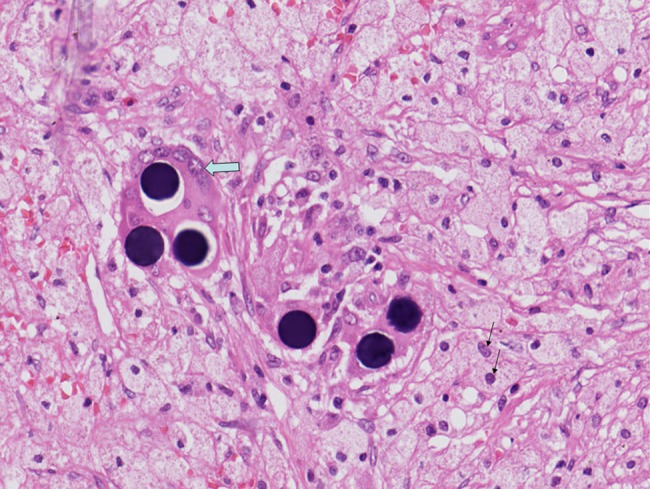
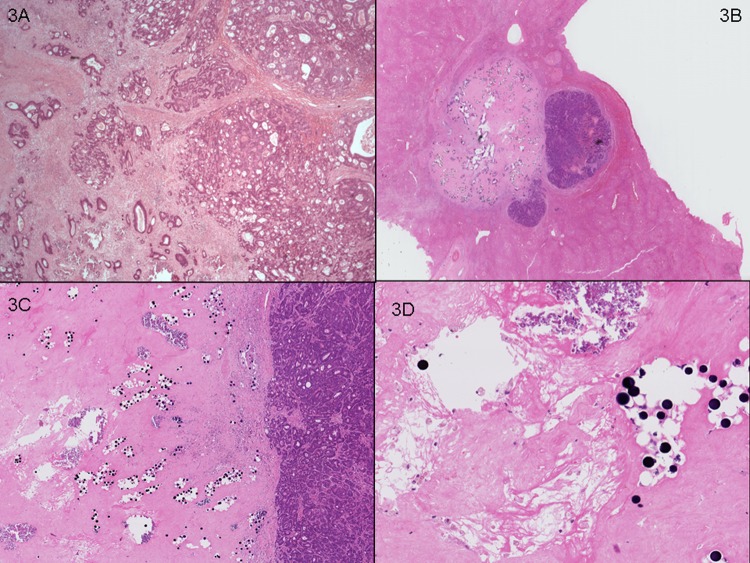
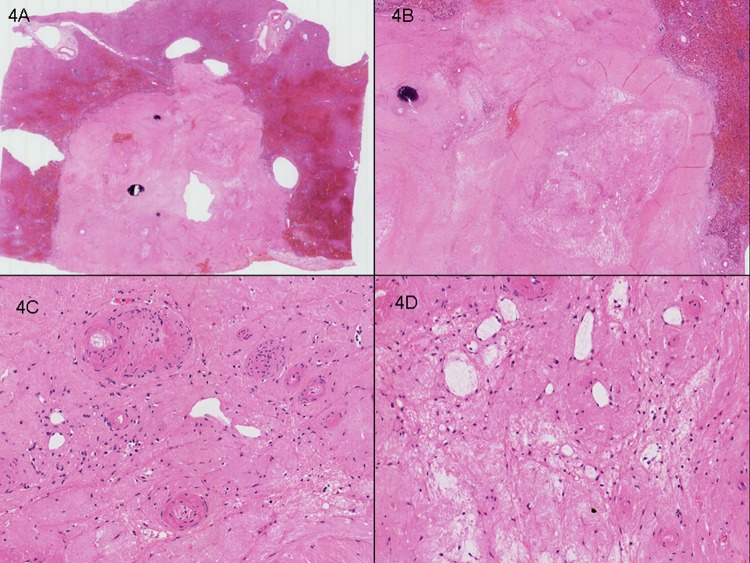
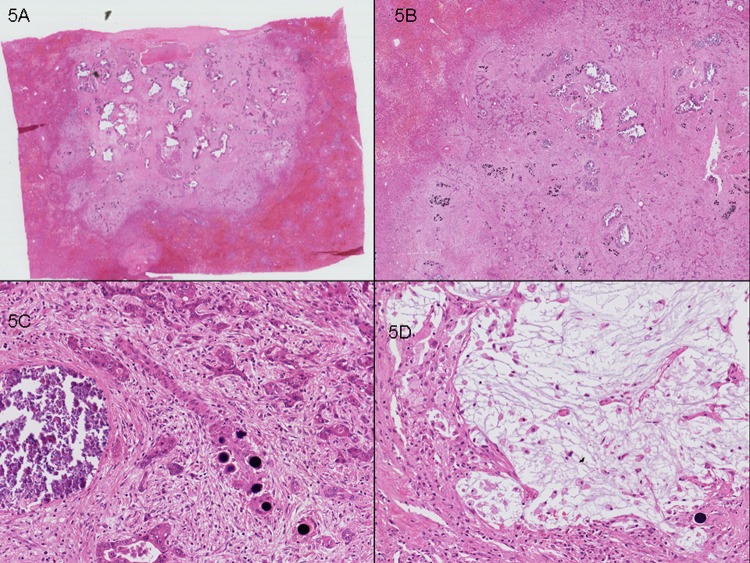
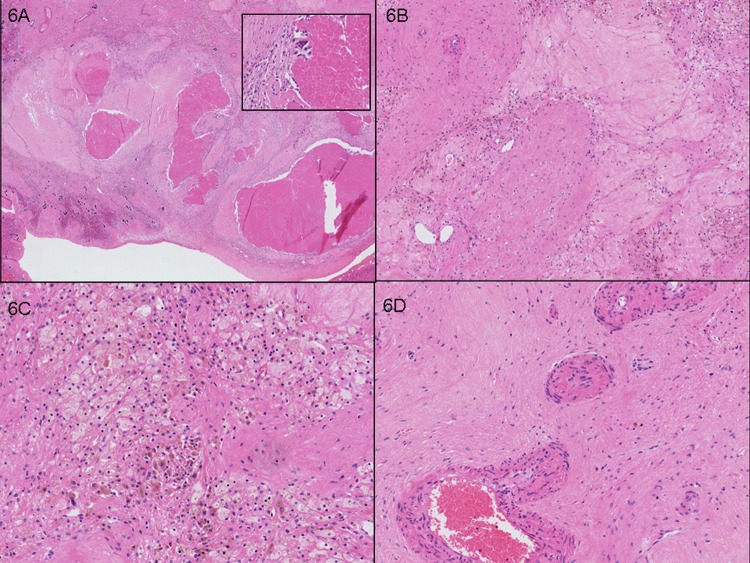
Results: Resin microspheres were identified in the vascular tumour bed and vessels within the portal tracts of the background liver parenchyma. Microspheres were usually associated with giant cell reaction or histiocytes. In the tumour bed, tumour necrosis, mucinous alteration, collections of foamy histiocytes, ectatic vessels, calcification and fibrosis were observed. There was minimal cellular inflammatory response observed, suggestive of direct radiation injury as a non-immune mediated process.
Conclusions: We describe in detail the spectrum of histopathological changes in malignant tissue and liver parenchyma in patients with metastatic CRC treated with SIRT. Our findings are consistent with the hypothesis that the principal mechanism of action of SIRT appears to be via arterially directed delivery of highly radioactive microspheres in and around the vascular tumour bed rather than by micro-arterial embolisation.
Figures
References
-
- Cabibbo G, Latteri F, Antonucci M, et al. Multimodal approaches to the treatment of hepatocellular carcinoma. Nat Clin Pract Gastroenterol Hepatol 2009;6:159–69 - PubMed
-
- Kerr D, McArdle C, Ledermann J, et al. Intrahepatic arterial versus intravenous fluorouracil and folinic acid for colorectal cancer liver metastases: a multicentre randomised trial. Lancet 2003;361:368–73 - PubMed
-
- Nicolay NH, Berry DP, Sharma RA. Liver metastases from colorectal cancer: radioembolization with systemic therapy. Nature Rev Clin Oncol 2009;6: 687–97 - PubMed
-
- Boerhaave H. Academical lectures on the theory of physic being. A genuine translation of his institutes and explanatory comment. London: W. Innys, 1774
-
- Willis RA. Mitosis in the hepatic metastases of malignant tumours. J Path & Bact 1932;35:11
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical