

Outcome of one-stage treatment of developmental dysplasia of hip in older children
- PMID: 23162148
- PMCID: PMC3491789
- DOI: 10.4103/0019-5413.101035
Outcome of one-stage treatment of developmental dysplasia of hip in older children
Abstract
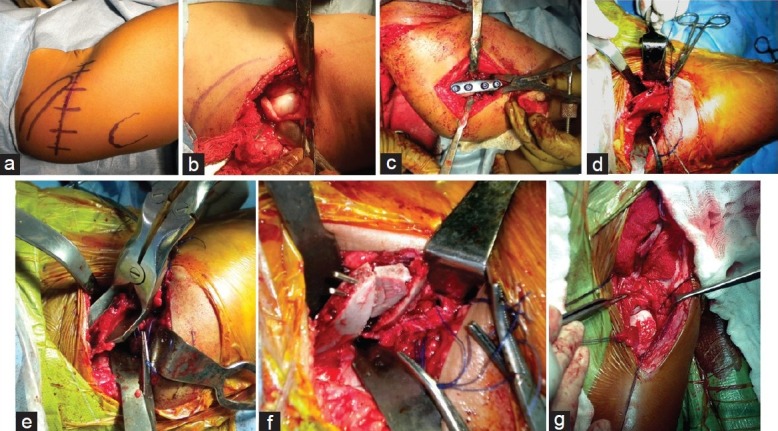
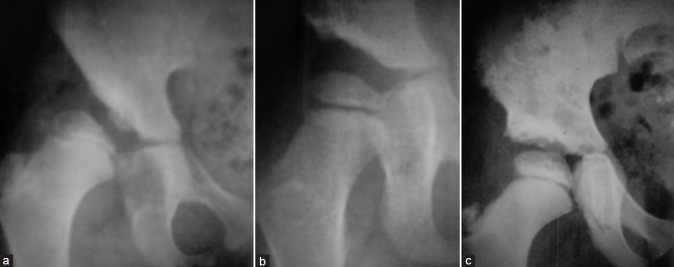
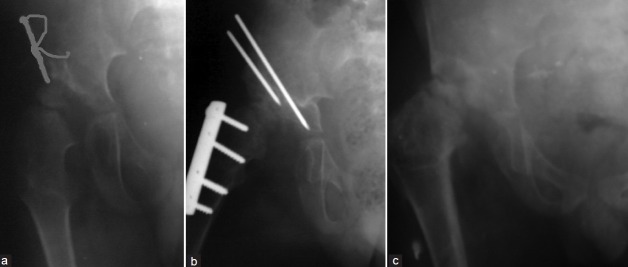
Background: The principles of treatment of congenital dislocation of hip in old children are different than those of infants and neonates. The purpose of this study is to evaluate the radiographic and functional results of one-stage treatment (open reduction, femoral shortening derotation, and Salter's osteotomy) of DDH in older children.
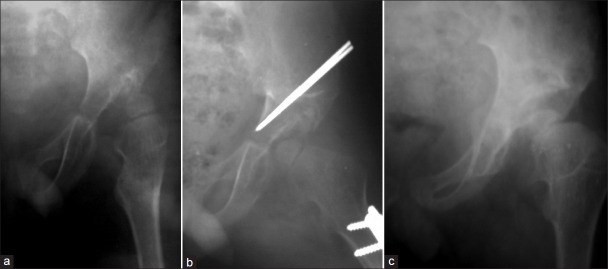
Materials and methods: Between January 2005 and June 2010, 25 patients (30 hips) underwent one-stage triple procedure of open reduction, femoral shortening derotation, and Salter's osteotomy for the treatment of DDH. Preoperatively, they were classified according to the Tönnis class. Clinical outcomes were assessed using the modified McKay's criteria to measure pain symptoms, gait pattern, Trendelenburg sign status, and the range of hip joint movement. Radiographic assessment was made using Severin's scoring method to measure the centre-edge angle and dysplasia.
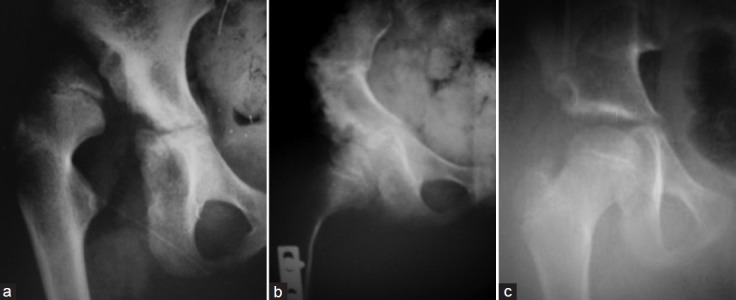
Results: The mean age at the time of operation was 3.9 years (range 1.6-8 years), and the average duration of followup was 4.1 years (range 2-7.6 years). The McKay's score was excellent in 13 hips, good in 14 hips, fair in 2, and poor in 1 hip. The Severin's class I and II was found in 25 (83.3%) hips at the time of final evaluation as compared to none at the time of presentation.
Conclusions: Young children having DDH can safely be treated with an extensive one-stage triple procedure of open reduction, femoral shortening derotation, and Salter's osteotomy, without increasing the risk of AVN. Early diagnosis and intervention is the successful treatment of patients suffering from DDH.
Keywords: Developmental dysplasia; derotation; femoral shortening; hip; salter's osteotomy.
Conflict of interest statement
Figures


Similar articles
-
Outcome of one stage combined open reduction, pelvic and derotation femoral osteotomy in congenital dislocated hips of children younger than three years age.J Pak Med Assoc. 2014 Sep;64(9):1015-20. J Pak Med Assoc. 2014. PMID: 25823180
-
Presentation and Management of Neglected Developmental Dysplasia of Hip (DDH): 8-years' experience with single stage triple procedure at National Institute of Rehabilitation Medicine, Islamabad, Pakistan.Pak J Med Sci. 2018 May-Jun;34(3):682-686. doi: 10.12669/pjms.343.14392. Pak J Med Sci. 2018. PMID: 30034439 Free PMC article.
-
Outcome of triple procedure in older children with developmental dysplasia of hip (DDH).J Pak Med Assoc. 2007 Dec;57(12):591-5. J Pak Med Assoc. 2007. PMID: 18173041
-
How Does Bony Surgery Affect Results of Anterior Open Reduction in Walking-age Children With Developmental Hip Dysplasia?Clin Orthop Relat Res. 2016 May;474(5):1199-208. doi: 10.1007/s11999-015-4598-x. Clin Orthop Relat Res. 2016. PMID: 26487045 Free PMC article. Review.
-
Cochrane Review: Screening programmes for developmental dysplasia of the hip in newborn infants.Evid Based Child Health. 2013 Jan;8(1):11-54. doi: 10.1002/ebch.1891. Evid Based Child Health. 2013. PMID: 23878122 Review.
Cited by
-
A Newly Modified Salter Osteotomy Technique for Treatment of Developmental Dysplasia of Hip That Is Associated with Decrease in Pressure on Femoral Head and Triradiate Cartilage.Biomed Res Int. 2019 Feb 6;2019:6021271. doi: 10.1155/2019/6021271. eCollection 2019. Biomed Res Int. 2019. PMID: 30881992 Free PMC article.
-
Open reduction and Salter innominate osteotomy combined with femoral osteotomy in the treatment of developmental dysplasia of the hip: Comparison of results before and after the age of 4 years.Acta Orthop Traumatol Turc. 2021 Jan;55(1):28-32. doi: 10.5152/j.aott.2021.17385. Acta Orthop Traumatol Turc. 2021. PMID: 33650507 Free PMC article.
-
Relapsed hip stiffness after recovery of range of motion in a hip treated for developmental dysplasia of the hip? Think again: A case report.Int J Surg Case Rep. 2020;77:843-847. doi: 10.1016/j.ijscr.2020.11.133. Epub 2020 Nov 30. Int J Surg Case Rep. 2020. PMID: 33395909 Free PMC article.
-
Management of developmental dysplasia of the hip in less than 24 months old children.Indian J Orthop. 2013 Nov;47(6):578-84. doi: 10.4103/0019-5413.121584. Indian J Orthop. 2013. PMID: 24379463 Free PMC article.
-
Accuracy of CT for measuring femoral neck anteversion in children with developmental dislocation of the hip verified using 3D printing technology.J Orthop Surg Res. 2021 Apr 14;16(1):256. doi: 10.1186/s13018-021-02400-x. J Orthop Surg Res. 2021. PMID: 33853657 Free PMC article.
References
-
- Klisic PJ. Congenital dislocation of the hip. A misleading term: Brief report. J Bone Joint Surg Br. 1989;71:136. - PubMed
-
- Beaty JH. Congenital and developmental anomalies of hip and pelvis. In: Canale ST, editor. Campbell's operative orthopedics. 11th ed. Philadelphia: Mosby; 2007. pp. 1180–220.
-
- Berkeley ME, Dickson JH, Cain TE, Donovan MM. Surgical therapy for congenital dislocation of the hip in patients who are twelve to thirty-six months old. J Bone Joint Surg Am. 1984;66:412–20. - PubMed
-
- Wedge JH, Wasylenko MJ. The natural history of congenital disease of the hip. J Bone Joint Surg Br. 1979;61:334–8. - PubMed
-
- Ashley RK, Larsen LJ, James PM. Reduction of dislocation of the hip in older children: A preliminary report. J Bone Joint Surg Am. 1972;54:545–50. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials