

Hemodynamic changes during robotic radical prostatectomy
- PMID: 23162392
- PMCID: PMC3498657
- DOI: 10.4103/1658-354X.101210
Hemodynamic changes during robotic radical prostatectomy
Abstract
Background: Effect on hemodynamic changes and experience of robot-assisted laparoscopic radical prostatectomy (RALRP) in steep Trendelenburg position (45°) with high-pressure CO(2) pneumoperitoneum is very limited. Therefore, we planned this prospective clinical trial to study the effect of steep Tredelenburg position with high-pressure CO(2) pneumoperitoneum on hemodynamic parameters in a patient undergoing RALRP using FloTrac/Vigileo™1.10.
Methods: After ethical approval and informed consent, 15 patients scheduled for RALRP were included in the study. In the operation room, after attaching standard monitors, the radial artery was cannulated. Anesthesia was induced with fentanyl (2 μg/kg) and thiopentone (4-7 mg/kg), and tracheal intubation was facilitated by vecuronium bromide (0.1 mg/kg). The patient's right internal jugular vein was cannulated and the Pre Sep™ central venous oximetry catheter was connected to it. Anesthesia was maintained with isoflurane in oxygen and nitrous oxide and intermittent boluses of vecuronium. Intermittent positive-pressure ventilation was provided to maintain normocapnea. After CO(2) pneumoperitoneum, position of the patient was gradually changed to 45° Trendelenburg over 5 min. The robot was then docked and the robot-assisted surgery started. Intraoperative monitoring included central venous pressure (CVP), stroke volume (SV), stroke volume variation (SVV), cardiac output (CO), cardiac index (CI) and central venous oxygen saturation (ScvO(2)).
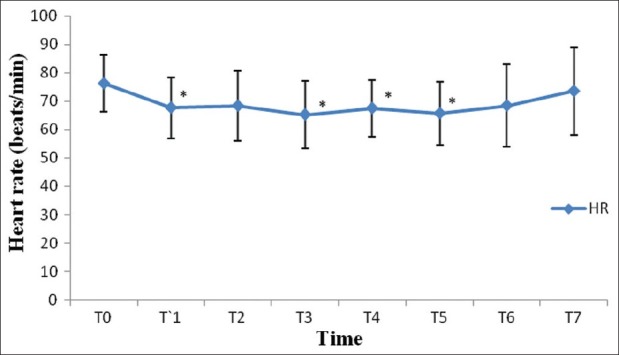
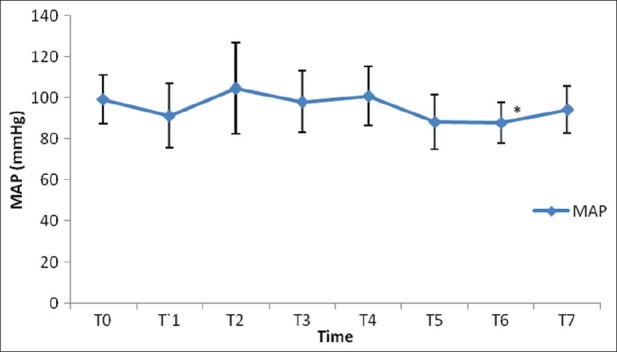
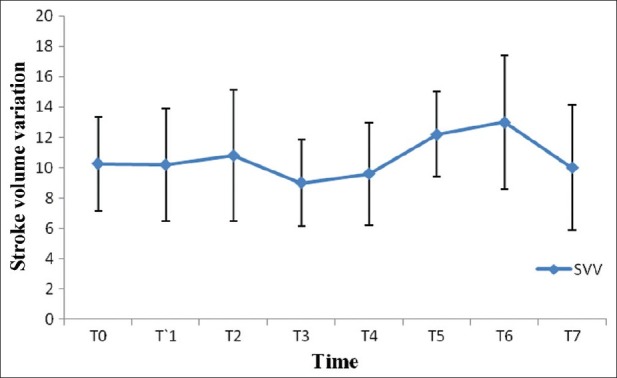
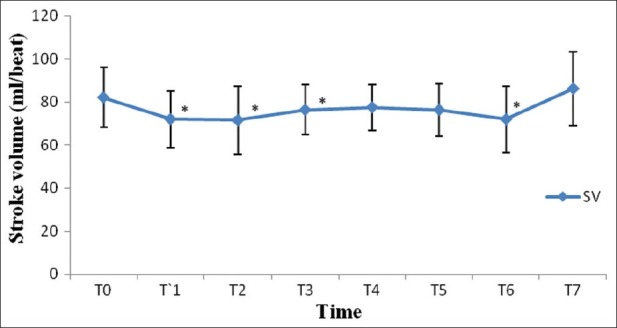
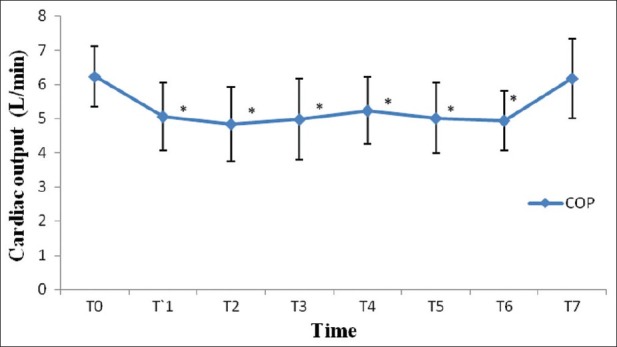
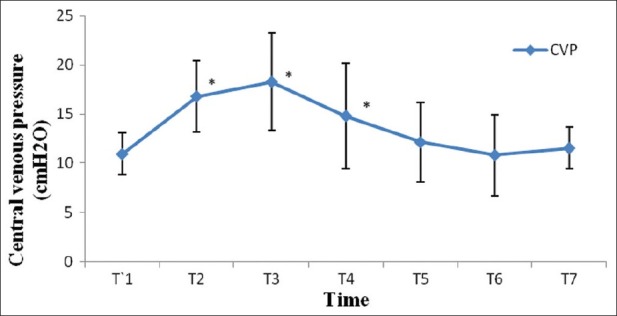
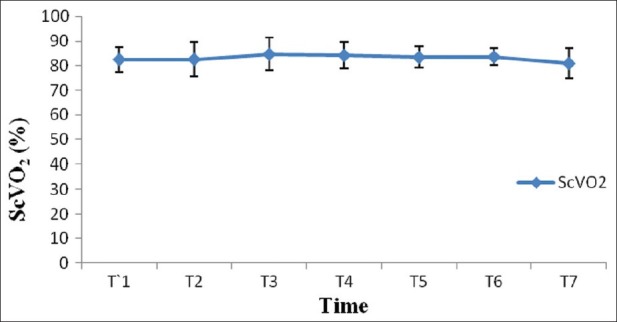
Results: After induction of anesthesia, heart rate (HR), SV, CO and CI were decreased significantly from the baseline value (P>0.05). SV, CO and CI further decreased significantly after creating pneumoperitoneum (P>0.05). At the 45° Trendelenburg position, HR, SV, CO and CI were significantly decreased compared with baseline. Thereafter, CO and CI were persistently low throughout the 45° Trendelenburg position (P=0.001). HR at 20 min and 1 h, SV and mean arterial blood pressure after 2 h decreased significantly from the baseline value (P>0.05) during the 45° Trendelenburg position. CVP increased significantly after creating pneumoperitoneum and at the 45° Trendelenburg position (after 5 and 20 min) compared with the baseline postinduction value (P>0.05). All these parameters returned to baseline after deflation of CO(2) pneumoperitoneum in the supine position. There were no significant changes in SVV and ScvO(2) throughout the study period.
Conclusions: The steep Trendelenburg position and CO(2) pneumoperitoneum, during RALRP, leads to significant decrease in stroke volume and cardiac output.
Keywords: Flotrac/vigileo™; hemodynamic changes; pneumoperitoneum; steep trendelenburg position.
Conflict of interest statement
Figures
Similar articles
-
Hemodynamic changes due to Trendelenburg positioning and pneumoperitoneum during laparoscopic hysterectomy.Acta Anaesthesiol Scand. 1995 Oct;39(7):949-55. doi: 10.1111/j.1399-6576.1995.tb04203.x. Acta Anaesthesiol Scand. 1995. PMID: 8848897
-
Hemodynamic perturbations during robot-assisted laparoscopic radical prostatectomy in 45° Trendelenburg position.Anesth Analg. 2011 Nov;113(5):1069-75. doi: 10.1213/ANE.0b013e3182075d1f. Epub 2011 Jan 13. Anesth Analg. 2011. PMID: 21233502
-
Sonographic optic nerve sheath diameter as a surrogate measure for intracranial pressure in anesthetized patients in the Trendelenburg position.BMC Anesthesiol. 2015 Mar 31;15:43. doi: 10.1186/s12871-015-0025-9. eCollection 2015. BMC Anesthesiol. 2015. PMID: 25861241 Free PMC article.
-
Challenges for anaesthesia for robotic-assisted surgery in the elderly: A narrative review.Eur J Anaesthesiol Intensive Care. 2023 Feb 9;2(2):e0019. doi: 10.1097/EA9.0000000000000019. eCollection 2023 Apr. Eur J Anaesthesiol Intensive Care. 2023. PMID: 39917591 Free PMC article. Review.
-
The Impact of Steep Trendelenburg Position on Intraocular Pressure.J Clin Med. 2022 May 18;11(10):2844. doi: 10.3390/jcm11102844. J Clin Med. 2022. PMID: 35628970 Free PMC article. Review.
Cited by
-
The effect of two different surgical positions on pulmonary functions ın laparoscopic sleeve gastrectomies: reverse Trendelenburg vs beach chair.Surg Endosc. 2025 Mar;39(3):1829-1838. doi: 10.1007/s00464-025-11538-2. Epub 2025 Jan 21. Surg Endosc. 2025. PMID: 39838149 Free PMC article. Clinical Trial.
-
Examining clinical outcomes utilizing low-pressure pneumoperitoneum during robotic-assisted radical prostatectomy.J Robot Surg. 2016 Sep;10(3):215-9. doi: 10.1007/s11701-016-0570-3. Epub 2016 Apr 8. J Robot Surg. 2016. PMID: 27059614
-
Anesthesia for robot-assisted surgery: a review.Anaesthesiol Intensive Ther. 2025 May 26;57(1):99-107. doi: 10.5114/ait/203168. Anaesthesiol Intensive Ther. 2025. PMID: 40420612 Free PMC article. Review.
-
Clinical Considerations and Outcomes of Robotic Urologic Surgery in Obese Patients.Turk J Anaesthesiol Reanim. 2024 May 3;52(2):39-48. doi: 10.4274/TJAR.2023.231315. Turk J Anaesthesiol Reanim. 2024. PMID: 38700096 Free PMC article.
-
Anesthetic considerations for robotic surgery.Korean J Anesthesiol. 2014 Jan;66(1):3-11. doi: 10.4097/kjae.2014.66.1.3. Epub 2014 Jan 28. Korean J Anesthesiol. 2014. PMID: 24567806 Free PMC article. Review.
References
-
- Cunningham AJ, Brull SJ. Laparoscopic cholecystectomy: Anaesthetic implications. Anesth Analg. 1993;76:1120–33. - PubMed
-
- Abbou CC, Hoznek A, Salomon L, Olsson LE, Lobontiu A, Saint F, et al. Laparoscopic radical prostatectomy with a remote controlled robot. J Urol. 2001;165:1964–6. - PubMed
-
- Koliopanos A, Zografos G, Skiathitis S, Stithos D, Voukena V, Karampinis A, et al. Esophageal Doppler (ODM II) improves intraoperative haemodynamic monitoring during laparoscopic surgery. Surg Laparosc Endosc Percutan Tech. 2005;15:332–8. - PubMed
-
- Myre K, Buanes T, Smith G, Stokland O. Simultaneous haemodynamic and echocardiographic changes during abdominal gas insufflation. Surg Laparosc Endosc. 1997;7:415–9. - PubMed
-
- O’Leary E, Hubbard K, Tormey W, Cunningham AJ. Laparoscopic cholecystectomy: Haemodynamic and neuroendocrine responses after CO2 pneumoperitoneum and changes in position. Br J Anaesth. 1996;76:640–4. - PubMed
