

Rationales for the Bernese approaches in acetabular surgery
- PMID: 23162669
- PMCID: PMC3495274
- DOI: 10.1007/s00068-012-0229-3
Rationales for the Bernese approaches in acetabular surgery
Abstract
Purpose: To present two new approaches to acetabular surgery that were established in Berne, and which aim at enhanced visualization and anatomical reconstruction of acetabular fractures.
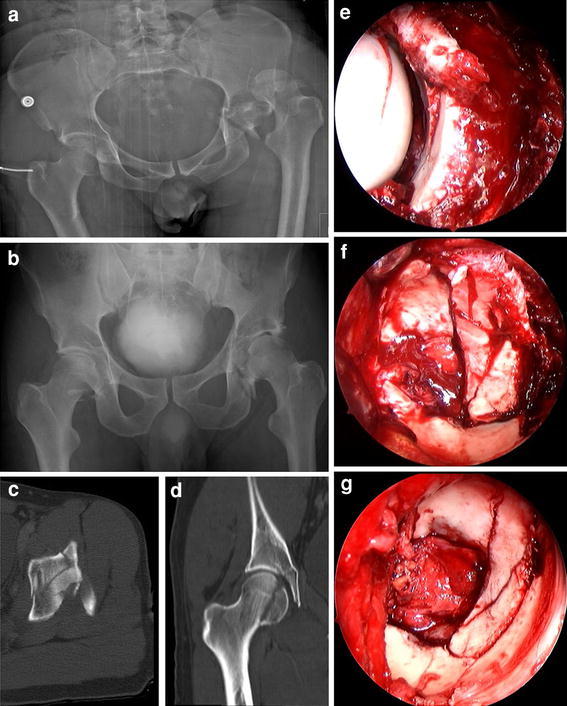
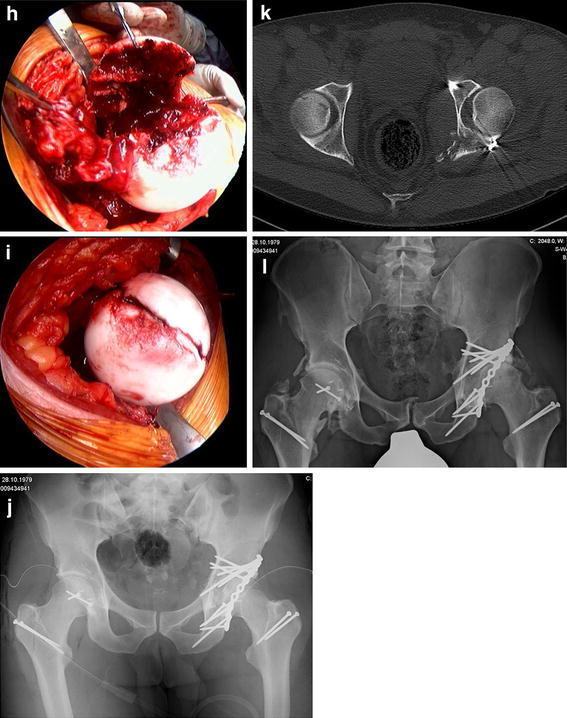
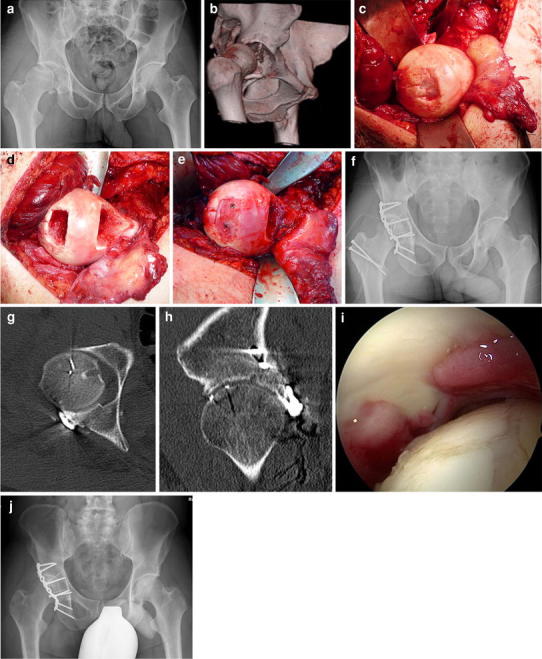
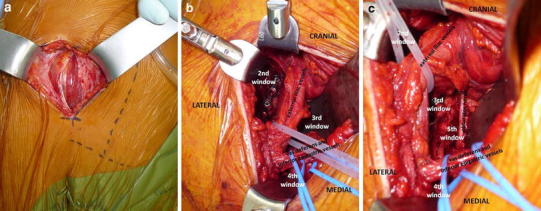
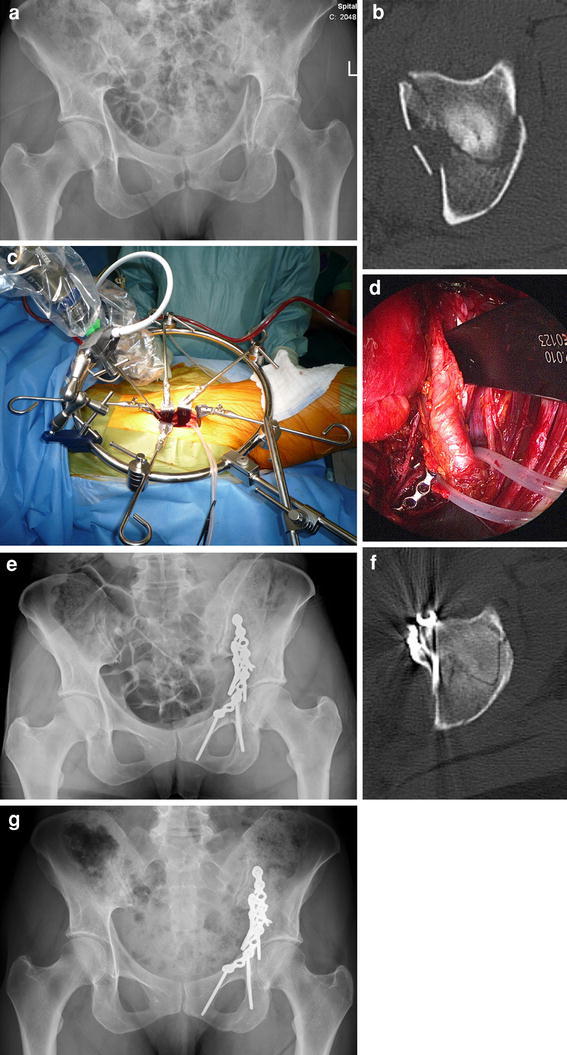
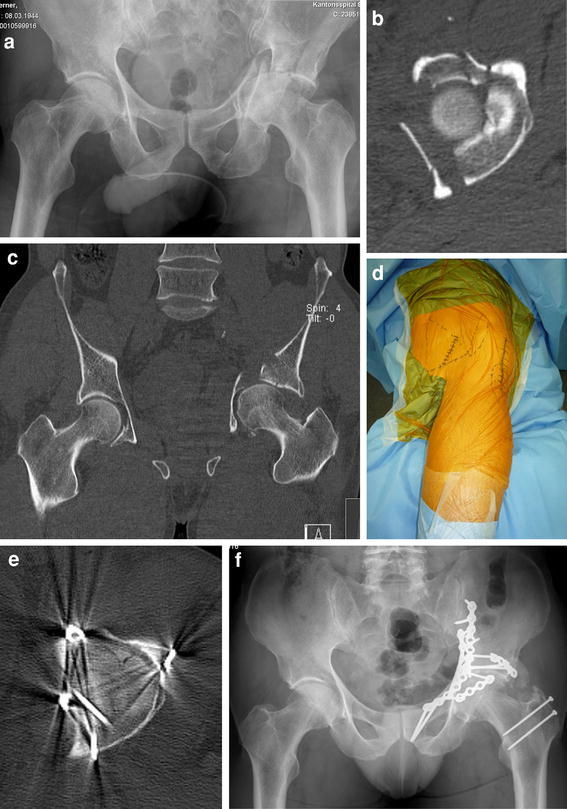
Method: The trochanteric flip osteotomy allows for surgical hip dislocation, and was introduced as a posterior approach for acetabular fracture management involving the posterior column and wall. For acetabular fractures predominantly involving the anterior column and the quadrilateral plate, the Pararectus approach is described.
Results: Full exposure of the hip joint, as provided by the trochanteric flip osteotomy, facilitates anatomical reduction of acetabular or femoral head fractures and safe positioning of the anterior column screw in transverse or T-shaped fractures. Additionally, the approach enables osteochondral transplantation as a salvage procedure for severe chondral femoral head damage and osteoplasty of an associated inadequate offset at the femoral head-neck junction. The Pararectus approach allows anatomical restoration with minimal access morbidity, and combines advantages of the ilioinguinal and modified Stoppa approaches.
Conclusions: Utilization of the trochanteric flip osteotomy eases visualization of the superior aspect of the acetabulum, and enables the evaluation and treatment of chondral lesions of the femoral head or acetabulum and labral tears. Displaced fractures of the anterior column with a medialized quadrilateral plate can be addressed successfully through the Pararectus approach, in which surgical access is associated with minimal morbidity. However, long-term results following the two presented Bernese approaches are needed to confirm that in the treatment of complex acetabular fractures the rate of poor results in almost one-third of all cases (as currently yielded using traditional approaches) might be reduced by the utilization of the presented novel approaches.
Figures
Similar articles
-
Internal fixation of anterior acetabular fractures with a limited pararectus approach and the anatomical plates: preliminary results.BMC Musculoskelet Disord. 2021 Feb 18;22(1):203. doi: 10.1186/s12891-021-04034-w. BMC Musculoskelet Disord. 2021. PMID: 33602187 Free PMC article.
-
[Surgical treatment of pelvic ring and acetabular fractures using the Stoppa approach].Acta Chir Orthop Traumatol Cech. 2010 Apr;77(2):93-8. Acta Chir Orthop Traumatol Cech. 2010. PMID: 20447350 Czech.
-
Digastric trochanteric flip osteotomy and surgical dislocation of hip in the management of acetabular fractures.Arch Orthop Trauma Surg. 2010 Jan;130(1):93-101. doi: 10.1007/s00402-009-0873-1. Arch Orthop Trauma Surg. 2010. PMID: 19373481
-
The Pararectus approach: a preferred surgical approach for fixation of acetabular fractures predominantly involving the anterior column - a narrative review.Arch Orthop Trauma Surg. 2024 Oct;144(10):4541-4547. doi: 10.1007/s00402-024-05455-7. Epub 2024 Jul 30. Arch Orthop Trauma Surg. 2024. PMID: 39078483 Free PMC article. Review.
-
[Research progress of different surgical approaches in treatment of acetabular both-column fractures].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021 Jun 15;35(6):661-666. doi: 10.7507/1002-1892.202012113. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021. PMID: 34142489 Free PMC article. Review. Chinese.
Cited by
-
Secure Screw Placement in Management of Acetabular Fractures Using the Suprapectineal Quadrilateral Buttress Plate.Biomed Res Int. 2017;2017:8231301. doi: 10.1155/2017/8231301. Epub 2017 Jun 15. Biomed Res Int. 2017. PMID: 28698880 Free PMC article.
-
The use of buttress plates in the management of acetabular fractures with quadrilateral plate involvement: is it still a valid option?Int Orthop. 2015 Nov;39(11):2219-26. doi: 10.1007/s00264-015-2883-7. Epub 2015 Jul 24. Int Orthop. 2015. PMID: 26206259
-
A systemic review and meta-analysis of pararectus versus ilioinguinal approach for the management of acetabular fractures.Eur J Orthop Surg Traumatol. 2024 Jan;34(1):549-560. doi: 10.1007/s00590-023-03700-0. Epub 2023 Aug 30. Eur J Orthop Surg Traumatol. 2024. PMID: 37646876
-
[Pelvic girdle and acetabulum].Unfallchirurg. 2013 Mar;116(3):196-7. doi: 10.1007/s00113-012-2328-3. Unfallchirurg. 2013. PMID: 23455846 German. No abstract available.
-
The infraacetabular screw versus the antegrade posterior column screw in acetabulum fractures with posterior column involvement: a biomechanical comparison.Arch Orthop Trauma Surg. 2024 Jun;144(6):2573-2582. doi: 10.1007/s00402-024-05324-3. Epub 2024 Apr 27. Arch Orthop Trauma Surg. 2024. PMID: 38676740 Free PMC article.
References
-
- Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J Bone Joint Surg (Br) 2005;87-B:2–9. - PubMed
-
- Letournel E. Acetabulum fractures: classification and management. Clin Orthop. 1980;151:81–106. - PubMed
-
- Anglen JO, Burd TA, Hendricks KJ, Harrision P. The “gull sign”: a harbinger of failure for internal fixation of geriatric acetabular fractures. J Orthop Trauma. 2003;17:625–34. - PubMed
