

Surgical results of patients with unilateral superior oblique palsy presenting with large hypertropias
- PMID: 23163258
- PMCID: PMC3606490
- DOI: 10.3928/01913913-20121113-01
Surgical results of patients with unilateral superior oblique palsy presenting with large hypertropias
Abstract
Purpose: Surgical management of superior oblique palsy (SOP) is challenging because of combined vertical, horizontal, and torsional misalignment. The authors report the surgical results of patients with large primary position hypertropias (> 20 prism diopters [PD]) due to unilateral SOP.
Methods: Criteria for success included correction of the anomalous head posture, primary position alignment between orthotropia and 6 PD of undercorrection, and no reoperation required for residual deviations in any direction of gaze.
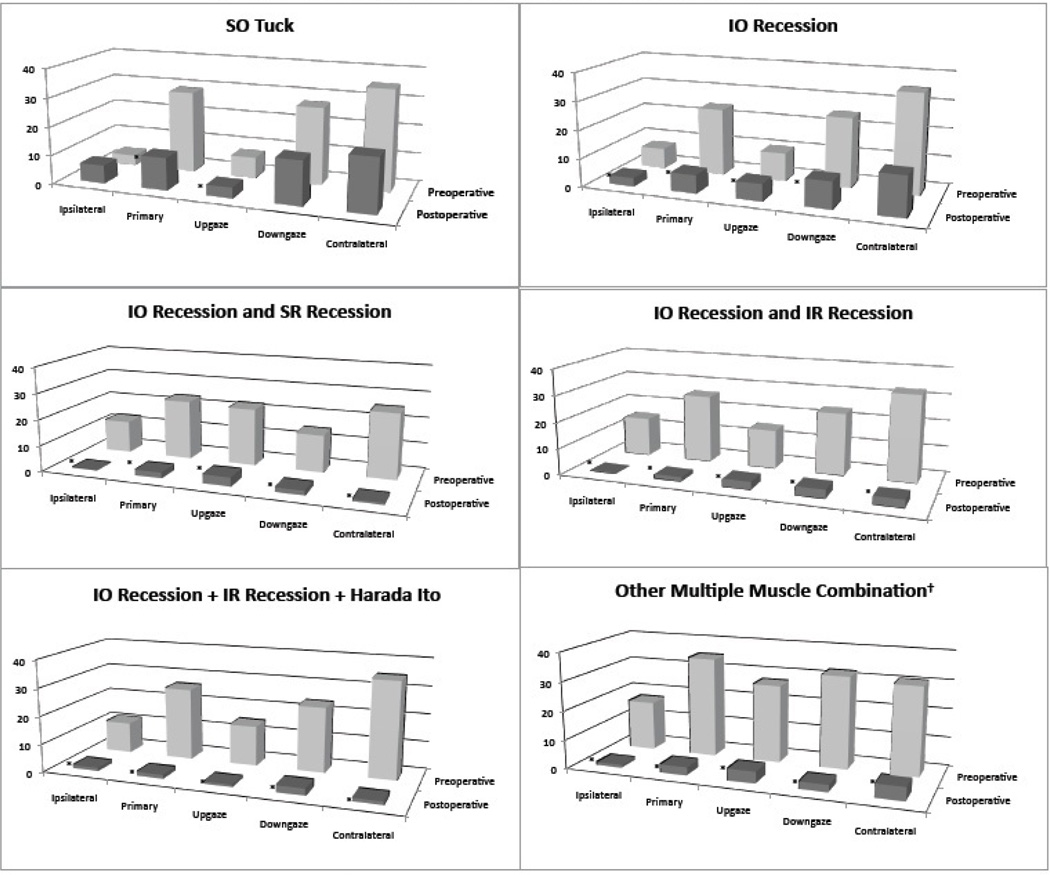
Results: Forty-five patients met inclusion criteria. Mean preoperative alignment in primary gaze was 26.5 ± 6.5 PD compared to 3.0 ± 4.4 PD postoperatively (P < .001). Twenty-three (51%) cases met the criteria for success with one operation. Of the patients who had single muscle surgery, 14% had a successful outcome, with a mean 67% (17.3 PD) reduction in hypertropia. Of patients who underwent simultaneous multiple muscle surgery, 58% met the criteria for a successful result, with a mean 92% (24.6 PD) reduction in primary gaze hypertropia. Success was the highest in patients who underwent ipsilateral inferior oblique combined with contralateral inferior rectus recessions with (60% success) or without (65% success) a Harada-Ito procedure.
Conclusion: Undercorrections are frequent following surgery for unilateral SOP with preoperative deviations greater than 20 PD in primary position, especially after single-muscle surgery. Simultaneous multiple muscle surgery rarely results in overcorrection and is recommended in patients with SOP and more than 20 PD of hypertropia in primary position.
Copyright 2013, SLACK Incorporated.
Figures
References
-
- Parks MM. Isolated cyclovertical muscle palsy. AMA Arch Ophthalmol. 1958;60:1027–1035. - PubMed
-
- Garnham L, Lawson JM, O’Neil D, et al. Botulinum toxin in fourth nerve palsies. Aust NZ J Ophthalmology. 1997;25:31–35. - PubMed
-
- Toosi SH, Von Noorden GK. Effect of isolated inferior oblique muscle myectomy in the management of superior oblique muscle palsy. Am J. Ophthalmol. 1979;88:602–608. - PubMed
-
- Jones TW, Lee DA, Dryer JA. Inferior oblique surgery: Experience at the Mayo Clinic from 1960 to 1981. Arch Ophthalmol. 1984;102:714–716. - PubMed
-
- Mulvihill A, Murphy M, Lee JP. Disinsertion of the inferior oblique muscle for treatment of superior oblique paresis. J Pediatr Ophthalmol Strabismus. 2000;37:279–282. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
