

Pediatric anti-N-methyl-D-aspartate receptor encephalitis-clinical analysis and novel findings in a series of 20 patients
- PMID: 23164315
- PMCID: PMC3582718
- DOI: 10.1016/j.jpeds.2012.10.011
Pediatric anti-N-methyl-D-aspartate receptor encephalitis-clinical analysis and novel findings in a series of 20 patients
Abstract
Objective: To report the clinical features of 20 pediatric patients with anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis.
Study design: Review of clinical data, long-term follow-up, and immunologic studies performed in a single center in Spain in the last 4 years.
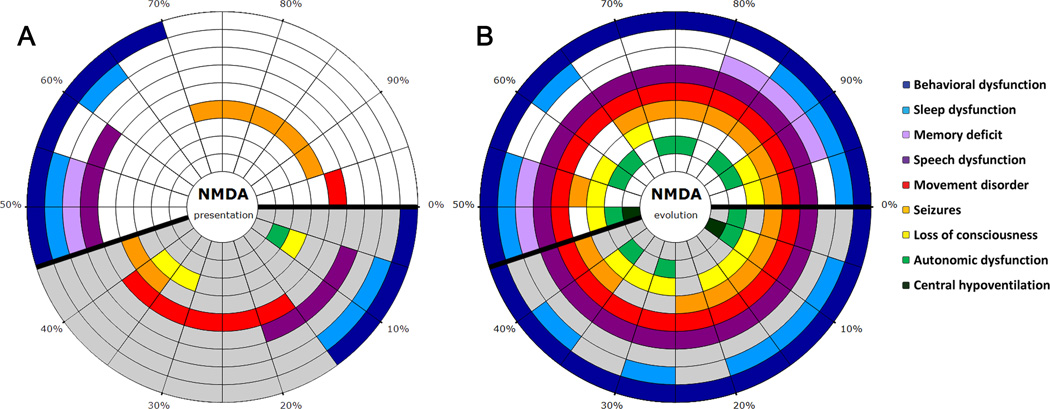
Results: The median age of the patients was 13 years (range, 8 months-18 years), 70% were female. In 12 patients (60%), the initial symptoms were neurologic, usually dyskinesias or seizures, and in the other 40% psychiatric. One month into the disease, all patients had involuntary movements and alterations of behavior and speech. All patients received steroids, intravenous immunoglobulin or plasma exchange, and 7 rituximab or cyclophosphamide. With a median follow up of 17.5 months, 85% had substantial recovery, 10% moderate or severe deficits, and 1 died. Three patients had previous episodes compatible with anti-NMDAR encephalitis, 2 of them with additional relapses after the diagnosis of the disorder. Ovarian teratoma was identified in 2 patients, 1 at onset of encephalitis and the other 1 year later. Two novel observations (1 patient each) include, the identification of an electroencephalographic pattern ("extreme delta brush") considered characteristic of this disorder, and the development of anti-NMDAR encephalitis as post herpes simplex encephalitis choreoathetosis.
Conclusions: The initial symptoms of pediatric anti-NMDAR encephalitis vary from those of the adults (more neurologic and less psychiatric in children), the development of a mono-symptomatic illness is extremely rare (except in relapses), and most patients respond to treatment. Our study suggests a link between post herpes simplex encephalitis choreoathetosis and anti-NMDAR encephalitis.
Copyright © 2013 Mosby, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Anti-N-methyl-D-aspartate receptor encephalitis: what's in a name?J Pediatr. 2013 Apr;162(4):673-5. doi: 10.1016/j.jpeds.2012.11.074. Epub 2013 Jan 8. J Pediatr. 2013. PMID: 23305956 No abstract available.
-
Anti-N-methyl-D-aspartate receptor encephalitis and parvovirus B19: A possible link?J Pediatr. 2013 Oct;163(4):1233-4. doi: 10.1016/j.jpeds.2013.06.079. Epub 2013 Aug 3. J Pediatr. 2013. PMID: 23919909 No abstract available.
References
-
- Granerod J, Ambrose HE, Davies NW, Clewley JP, Walsh AL, Morgan D, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis. 2010;10:835–844. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
