

Thyroid nodules in pediatrics: which ones can be left alone, which ones must be investigated, when and how
- PMID: 23165002
- PMCID: PMC3608010
- DOI: 10.4274/jcrpe.853
Thyroid nodules in pediatrics: which ones can be left alone, which ones must be investigated, when and how
Abstract
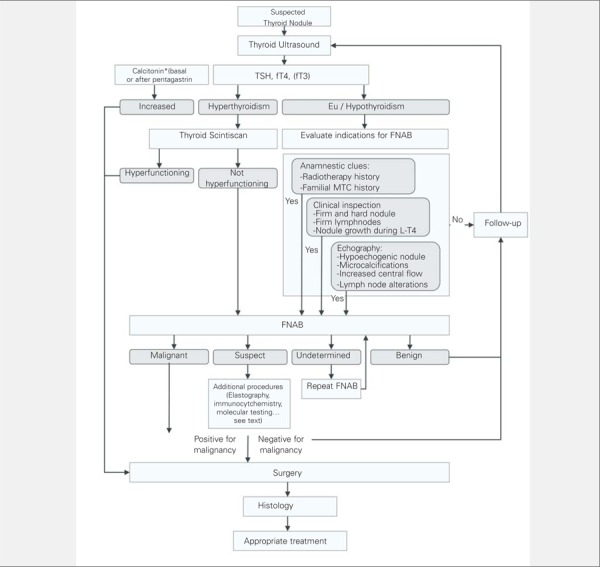
Thyroid nodules are less frequent in childhood than in adulthood, but are more often malignant. Recent estimates suggest that up to 25% of thyroid nodules in children are malignant, therefore, a more aggressive approach is recommended. In this review, we suggest an approach based on a first-step clinical, laboratory, and sonographic evaluation. A history of irradiation of the neck, cranium or upper thorax, previous thyroid diseases or thyroid neoplasms in the family should alert clinicians as being associated with a greater likelihood of malignant nodules. Signs or symptoms of hyperthyroidism and dysmorphic features should be carefully considered during the physical examination. Palpable firm lymph nodes, found in some 70% of cases, are the most significant clinical finding in children with malignant nodules. Although the routine determination of calcitonin levels is not uniformly practiced, it can help recognize sporadic or familial medullary thyroid neoplasms. Blood thyroid stimulating hormone, free thyroxine, and free triiodothyronine determinations (the latter in case of symptoms of hyperthyroidism) are aimed at identifying the few hyperthyroid patients, for whom the next step should be scintiscan. Hyperthyroid patients usually disclose an increased uptake, and a diagnosis of toxic adenoma is commonly made. Cases with normal thyroid function or hypothyroidism (which is usually subclinical) should be evaluated by fine-needle aspiration biopsy (FNAB). In eu/hypo-thyroid patients, scintiscan provides poor diagnostic information and should not be routinely employed. Thyroid ultrasonography is used to select cases for FNAB. Although ultrasound cannot reliably discriminate between benign and malignant lesions, it does provide an index of suspicion. Sonographic features that increase the likelihood of malignancy are microcalcifications, lymph node alterations, nodule growth under levothyroxine treatment, and increased intranodular vascularization demonstrated by color Doppler. There is growing evidence that elastography may provide further information on nodule characteristics. FNAB is indicated in all cases with a likelihood of malignancy. FNAB has a diagnostic accuracy of approximately 90% and is used in selection of patients which require surgery. Recently, histological markers and elastography have been introduced to increase the specificity of FNAB and ultrasound, respectively. The pitfall in FNAB cytology is the follicular cytology, in which it is not possible to distinguish between adenoma and carcinoma and therefore thyroidectomy is advised.
Figures
Similar articles
-
Diagnostic features of thyroid nodules in pediatrics.Arch Pediatr Adolesc Med. 2010 Aug;164(8):714-9. doi: 10.1001/archpediatrics.2010.114. Arch Pediatr Adolesc Med. 2010. PMID: 20679162
-
The rational use of fine needle aspiration biopsy (FNAB) in diagnosing thyroid nodules.Minerva Endocrinol. 2006 Jun;31(2):159-72. Minerva Endocrinol. 2006. PMID: 16682939 English, Italian.
-
Predictors of Malignancy in Children with Thyroid Nodules.J Pediatr. 2015 Oct;167(4):886-892.e1. doi: 10.1016/j.jpeds.2015.06.026. Epub 2015 Jul 8. J Pediatr. 2015. PMID: 26164379
-
Pediatric thyroid nodules: insights in management.Bol Asoc Med P R. 1998 Apr-Jun;90(4-6):74-8. Bol Asoc Med P R. 1998. PMID: 9866271 Review.
-
Controversies in the management of cold, hot, and occult thyroid nodules.Am J Med. 1995 Dec;99(6):642-50. doi: 10.1016/s0002-9343(99)80252-6. Am J Med. 1995. PMID: 7503088 Review.
Cited by
-
Thyroid nodules in children and adolescents: Investigation and management.J Paediatr Child Health. 2022 Dec;58(12):2163-2168. doi: 10.1111/jpc.16257. Epub 2022 Nov 16. J Paediatr Child Health. 2022. PMID: 36382588 Free PMC article. Review.
-
Risk factors of recurrent thyroid nodules after radiofrequency ablation.Afr Health Sci. 2023 Sep;23(3):584-592. doi: 10.4314/ahs.v23i3.68. Afr Health Sci. 2023. PMID: 38357154 Free PMC article.
-
The Clinical and Pathological Presentation of Thyroid Nodules in Children and the Comparison with Adult Population: Experience of a Single Institution.Int J Endocrinol. 2016;2016:1256189. doi: 10.1155/2016/1256189. Epub 2016 Mar 20. Int J Endocrinol. 2016. PMID: 27087807 Free PMC article.
-
Histopathological profile of childhood thyroid carcinoma in Ibadan, Southwestern Nigeria.Malawi Med J. 2020 Dec;32(4):213-217. doi: 10.4314/mmj.v32i4.6. Malawi Med J. 2020. PMID: 34457206 Free PMC article.
-
Evaluation of the efficacy of EU-TIRADS and ACR-TIRADS in risk stratification of pediatric patients with thyroid nodules.Front Endocrinol (Lausanne). 2022 Nov 22;13:1041464. doi: 10.3389/fendo.2022.1041464. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36482990 Free PMC article.
References
-
- Dean DS, Gharib H. Epidemiology of thyroid nodules. Best Pract Res Clin Endocrinol Metab. 2008;22:901–911. - PubMed
-
- Rallison ML, Dobyns BM, Keating FR Jr, Rall JE, Tyler FH. Thyroid nodularity in children. JAMA. 1975;233:1069–1072. - PubMed
-
- 3. Corrias A, Mussa A, Baronio F, Arrigo T, Salerno M, Segni M, Vigone MC, Gastaldi R, Zirilli G, Tuli G, Beccaria L, Iughetti L, Einaudi S, Weber G, De Luca F. Diagnostic features of thyroid nodules in pediatrics. Arch Pediatr Adolesc Med. 2010;164:714–719. - PubMed
-
- Niedziela M. Pathogenesis, diagnosis and management of thyroid nodules in children. Endocr Relat Cancer. 2006;13:427–453. - PubMed
-
- 5. Aghini-Lombardi F, Antonangeli L, Martino E, Vitti P, Maccherini D, Leoli F, Rago T, Grasso L, Valeriano R, Balestrieri A, Pinchera A. The spectrum of thyroid disorders in an iodine-deficient community:the Pescopagano survey. J Clin Endocrinol Metab. 1999;84:561–566. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources