

Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter
- PMID: 23165462
- PMCID: PMC3553731
- DOI: 10.1128/AAC.01568-12
Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter
Abstract
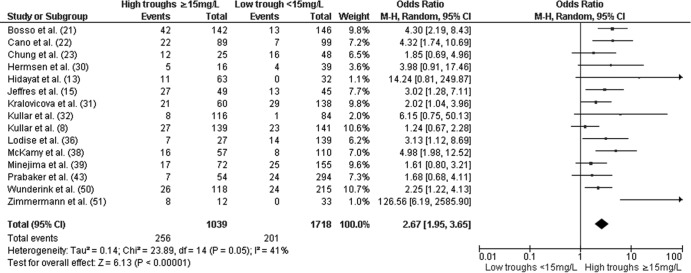
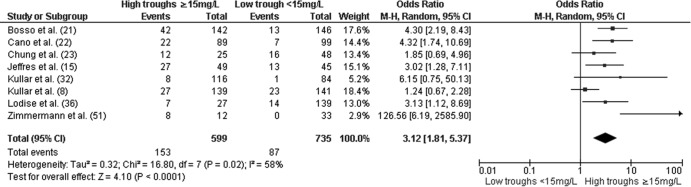
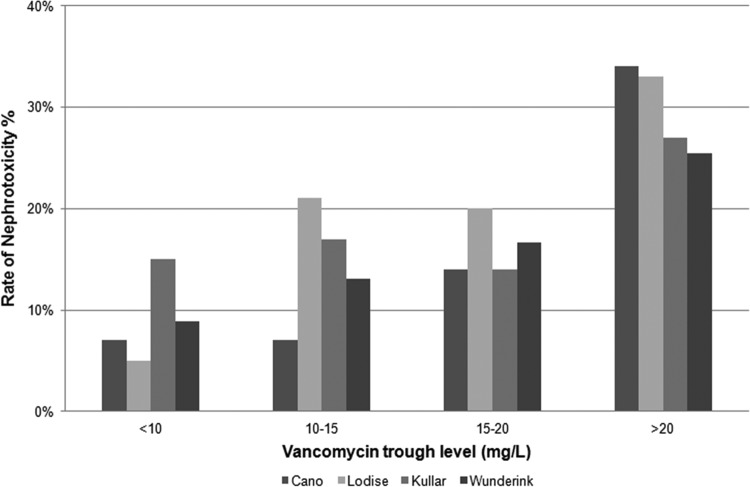
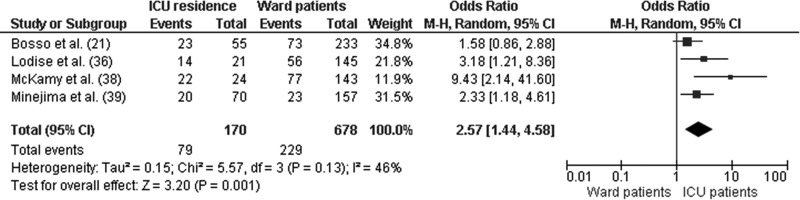
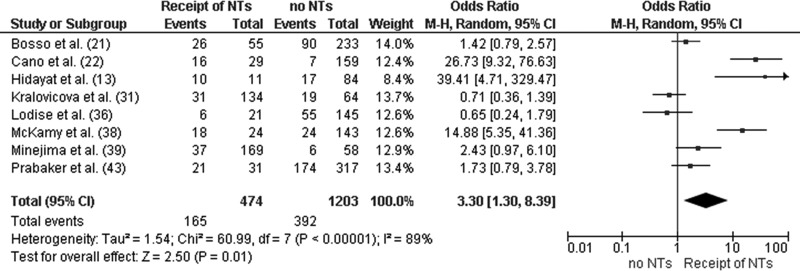
In an effort to maximize outcomes, recent expert guidelines recommend more-intensive vancomycin dosing schedules to maintain vancomycin troughs between 15 and 20 mg/liter. The widespread use of these more-intensive regimens has been associated with an increase in vancomycin-induced nephrotoxicity reports. The purpose of this systematic literature review is to determine the nephrotoxicity potential of maintaining higher troughs in clinical practice. All studies pertaining to vancomycin-induced nephrotoxicity between 1996 and April 2012 were identified from PubMed, Embase, Cochrane Controlled Trial Registry, and Medline databases and analyzed according to Cochrane guidelines. Of the initial 240 studies identified, 38 were reviewed, and 15 studies met the inclusion criteria. Overall, higher troughs (≥ 15 mg/liter) were associated with increased odds of nephrotoxicity (odds ratio [OR], 2.67; 95% confidence interval [CI], 1.95 to 3.65) relative to lower troughs of <15 mg/liter. The relationship between a trough of ≥ 15 mg/liter and nephrotoxicity persisted when the analysis was restricted to studies that examined only initial trough concentrations (OR, 3.12; 95% CI, 1.81 to 5.37). The relationship between troughs of ≥ 15 mg/liter and nephrotoxicity persisted after adjustment for covariates known to independently increase the risk of a nephrotoxicity event. An incremental increase in nephrotoxicity was also observed with longer durations of vancomycin administration. Vancomycin-induced nephrotoxicity was reversible in the majority of cases, with short-term dialysis required only in 3% of nephrotoxic episodes. The collective literature indicates that an exposure-nephrotoxicity relationship for vancomycin exists. The probability of a nephrotoxic event increased as a function of the trough concentration and duration of therapy.
Figures
Comment in
-
Vancomycin-induced nephrotoxicity.Antimicrob Agents Chemother. 2013 May;57(5):2435. doi: 10.1128/AAC.00253-13. Antimicrob Agents Chemother. 2013. PMID: 23580581 Free PMC article. No abstract available.
-
Reply to "Vancomycin-induced nephrotoxicity".Antimicrob Agents Chemother. 2013 May;57(5):2436. doi: 10.1128/AAC.00320-13. Antimicrob Agents Chemother. 2013. PMID: 23580582 Free PMC article. No abstract available.
References
-
- Levine DP. 2006. Vancomycin: a history. Clin. Infect. Dis. 42(Suppl 1):S5–S12 - PubMed
-
- Popovich KJ, Weinstein RA, Hota B. 2008. Are community-associated methicillin-resistant Staphylococcus aureus (MRSA) strains replacing traditional nosocomial MRSA strains? Clin. Infect. Dis. 46:787–794 - PubMed
-
- Naimi TS, LeDell KH, Como-Sabetti K, Borchardt SM, Boxrud DJ, Etienne J, Johnson SK, Vandenesch F, Fridkin S, O'Boyle C, Danila RN, Lynfield R. 2003. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA 290:2976–2984 - PubMed
-
- Fridkin SK, Hageman JC, Morrison M, Sanza LT, Como-Sabetti K, Jernigan JA, Harriman K, Harrison LH, Lynfield R, Farley MM. 2005. Methicillin-resistant Staphylococcus aureus disease in three communities. N. Engl. J. Med. 352:1436–1444 - PubMed
-
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, Talan M JRDA, Chambers HF. 2011. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 52:e18–e55 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
