

Postoperative mortality after surgery for brain tumors by patient insurance status in the United States
- PMID: 23165616
- PMCID: PMC3571758
- DOI: 10.1001/archsurg.2012.1459
Postoperative mortality after surgery for brain tumors by patient insurance status in the United States
Abstract
Objective: To examine whether being uninsured is associated with higher in-hospital postoperative mortality when undergoing surgery in the United States for a brain tumor.
Design: Retrospective cohort study using the Nationwide Inpatient Sample, January 1, 1999, through December 31, 2008.
Setting: The Nationwide Inpatient Sample contains all inpatient records from a stratified sample of 20% of hospitals in 37 states.
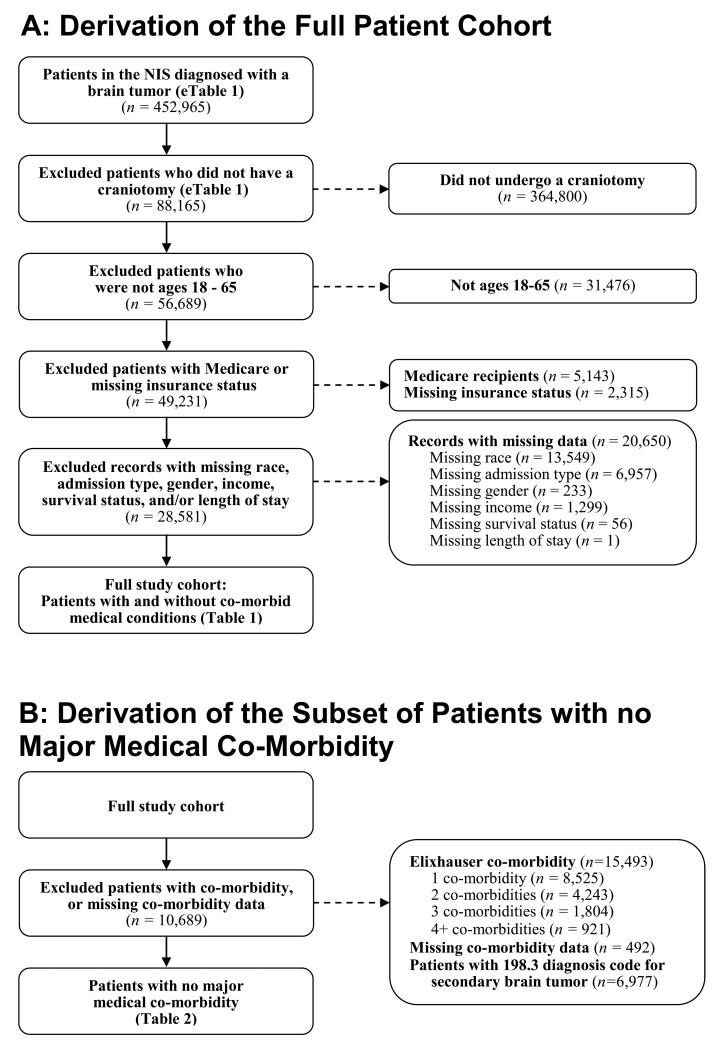
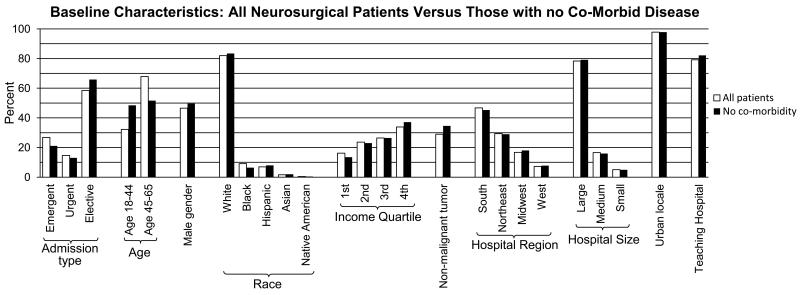
Patients: A total of 28,581 patients, aged 18 to 65 years, who underwent craniotomy for a brain tumor. Three groups were studied: Medicaid recipients and privately insured and uninsured patients.
Main outcome measure: The main outcome measure was in-hospital postoperative death. Associations between this outcome and insurance status were examined within the full cohort and within the subset of patients with no comorbidity using Cox proportional hazards models. These models were stratified by hospital to control for any clustering effects that could arise from differing access to care.
Results: In the unadjusted analysis, the mortality rate for privately insured patients was 1.3% (95% CI, 1.1%-1.4%) compared with 2.6% for uninsured patients (95% CI, 1.9%-3.3%; P < .001) and 2.3% for Medicaid recipients (95% CI, 1.8%-2.8%; P < .001). After adjusting for patient characteristics and stratifying by hospital in patients with no comorbidity, uninsured patients still had a higher risk of experiencing in-hospital death (hazard ratio, 2.62; 95% CI, 1.11-6.14; P = .03) compared with privately insured patients. In this adjusted analysis, the disparity was not conclusively present in Medicaid recipients (hazard ratio, 2.03; 95% CI, 0.97-4.23; P = .06).
Conclusions: Uninsured patients who underwent craniotomy for a brain tumor experienced the highest in-hospital mortality. Differences in overall health do not fully account for this disparity.
Figures
Comment in
-
Is insurance status a modifiable factor in brain tumor treatment outcomes?: comment on "Postoperative mortality after surgery for brain tumors by patient insurance status in the United States".Arch Surg. 2012 Nov;147(11):1025. doi: 10.1001/archsurg.2012.1493. Arch Surg. 2012. PMID: 23165617 No abstract available.
References
-
- Barker FG, 2nd, Klibanski A, Swearingen B. Transsphenoidal surgery for pituitary tumors in the United States, 1996-2000: mortality, morbidity, and the effects of hospital and surgeon volume. J Clin Endocrinol Metab. 2003 Oct;88(10):4709, 4719. - PubMed
-
- Kelz RR, Gimotty PA, Polsky D, Norman S, Fraker D, DeMichele A. Morbidity and mortality of colorectal carcinoma surgery differs by insurance status. Cancer. 2004 Nov 15;101(10):2187–2194. - PubMed
-
- American Cancer Society . Cancer Facts & Figures 2010. American Cancer Society; Atlanta: 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
