

Disentangling the effects of risk factors and clinical care on subnational variation in early neonatal mortality in the United States
- PMID: 23166659
- PMCID: PMC3498121
- DOI: 10.1371/journal.pone.0049399
Disentangling the effects of risk factors and clinical care on subnational variation in early neonatal mortality in the United States
Abstract
Objective: Between 1990 and 2010, the U.S ranking in neonatal mortality slipped from 29(th) to 45(th) among countries globally. Substantial subnational variation in newborn mortality also exists. Our objective is to measure the extent to which trends and subnational variation in early neonatal mortality reflect differences in the prevalence of risk factors (gestational age and birth weight) compared to differences in clinical care.
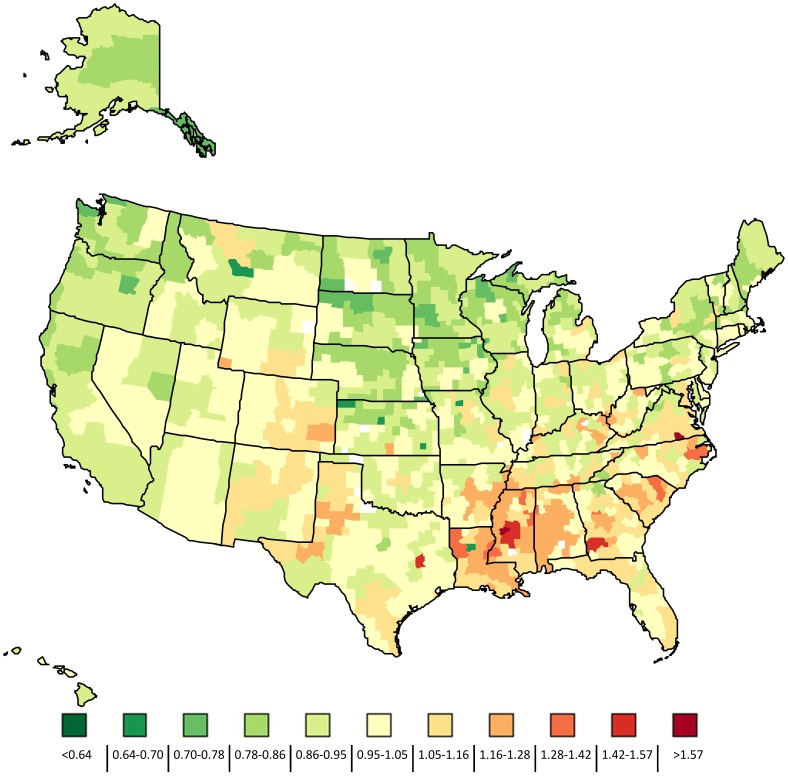
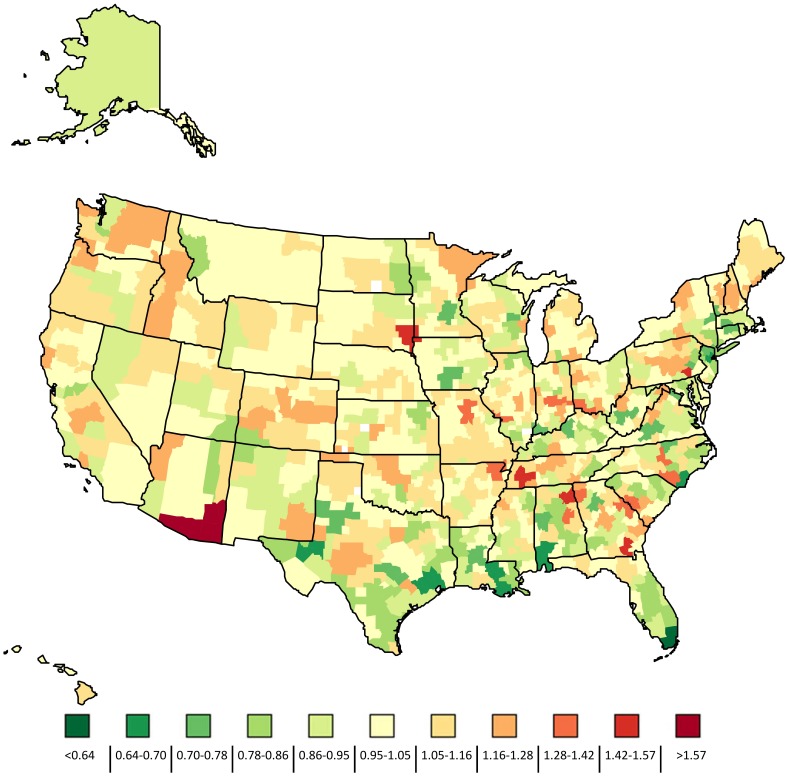
Methods: Observational study using linked birth and death data for all births in the United States between 1996 and 2006. We examined health service area (HSA) level variation in the expected early neonatal mortality rate, based on gestational age (GA) and birth-weight (BW), and GA-BW adjusted mortality as a proxy for clinical care. We analyzed the relationship between selected health system indicators and GA-BW-adjusted mortality.
Results: The early neonatal death (ENND) rate declined 12% between 1996 and 2006 (2.39 to 2.10 per 1000 live births). This occurred despite increases in risk factor prevalence. There was significant HSA-level variation in the expected ENND rate (Rate Ratio: 0.73-1.47) and the GA-BW adjusted rate (Rate ratio: 0.63-1.68). Accounting for preterm volume (defined as <34 weeks), the number of neonatologist and NICU beds, 25.2% and 58.7% of the HSA-level variance in outcomes was explained among all births and very low birth weight babies, respectively.
Conclusion: Improvements in mortality could be realized through the expansion or reallocation of clinical neonatal resources, particularly in HSAs with a high volume of preterm births; however, prevention of preterm births and low-birth weight babies has a greater potential to improve newborn survival in the United States.
Conflict of interest statement
Figures

References
-
- Lozano R, Wang H, Foreman KJ, Rajaratnam JK, Naghavi M, et al. (2011) Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. The Lancet 378: 1139–1165 doi:10.1016/S0140-6736(11)61337–8 - DOI - PubMed
-
- Murray CJL, Kulkarni SC, Michaud C, Tomijima N, Bulzacchelli MT, et al. (2006) Eight Americas: Investigating Mortality Disparities across Races, Counties, and Race-Counties in the United States. PLoS Med 3: e260 doi:10.1371/journal.pmed.0030260 - DOI - PMC - PubMed
-
- Deaths: final data for 2006 (2009) Centers for Disease Control and Prevention, National Center for Health Statistics. - PubMed
-
- Dietz PM, England LJ, Shapiro-Mendoza CK, Tong VT, Farr SL, et al. (2010) Infant morbidity and mortality attributable to prenatal smoking in the U.S. Am J Prev Med. 39: 45–52 doi:10.1016/j.amepre.2010.03.009 - DOI - PubMed
-
- Salihu HM, Aliyu MH, Pierre-Louis BJ, Alexander GR (2003) Levels of excess infant deaths attributable to maternal smoking during pregnancy in the United States. Matern Child Health J 7: 219–227. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
