

Projecting the long-term impact of school- or community-based mass-treatment interventions for control of Schistosoma infection
- PMID: 23166850
- PMCID: PMC3499404
- DOI: 10.1371/journal.pntd.0001903
Projecting the long-term impact of school- or community-based mass-treatment interventions for control of Schistosoma infection
Abstract
Background: Schistosomiasis remains a significant health burden in many areas of the world. Morbidity control, focused on limiting infection intensity through periodic delivery of anti-schistosomal medicines, is the thrust of current World Health Organization guidelines (2006) for reduction of Schistosoma-related disease. A new appreciation of the lifetime impact of repeated Schistosoma infection has directed attention toward strategies for greater suppression of parasite infection per se, with the goal of transmission interruption. Variations in drug schedules involving increased population coverage and/or treatment frequency are now undergoing field trials. However, their relative effectiveness in long-term infection suppression is presently unknown.
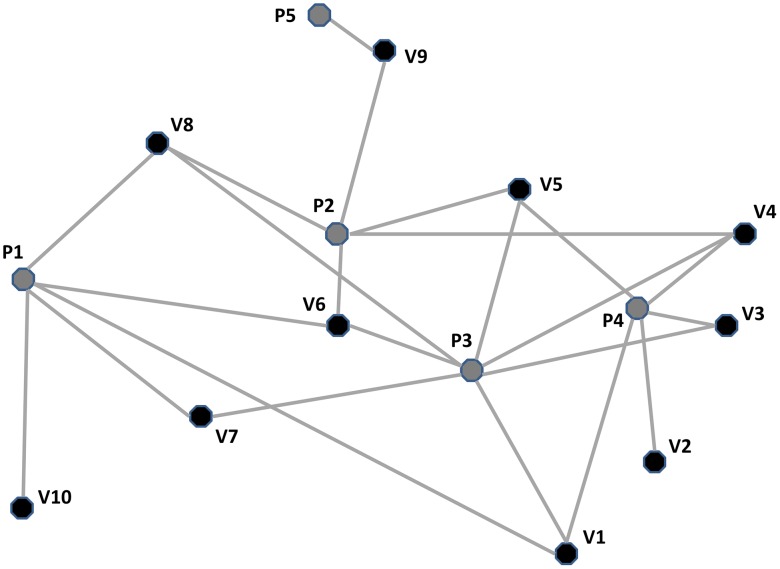
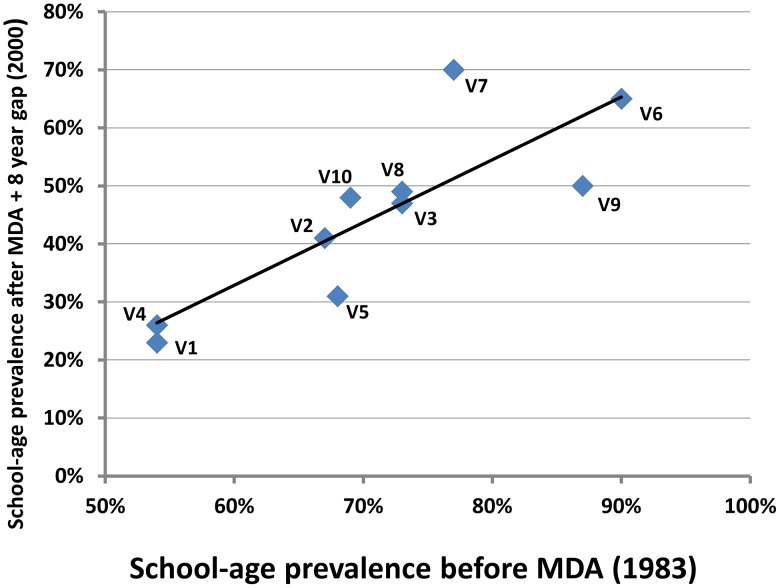
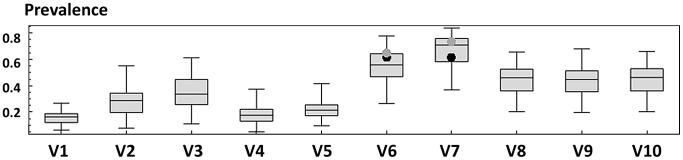
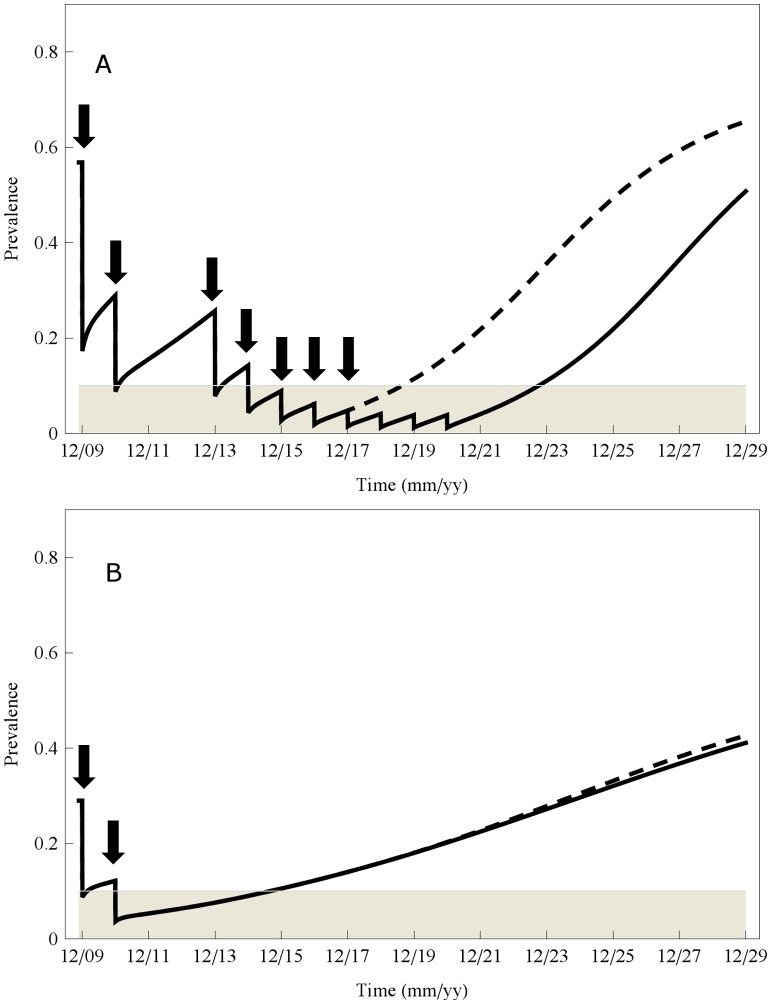
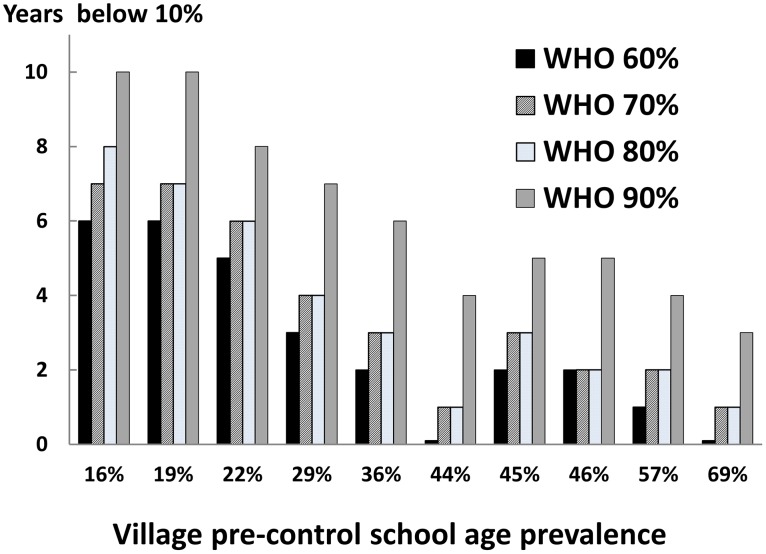
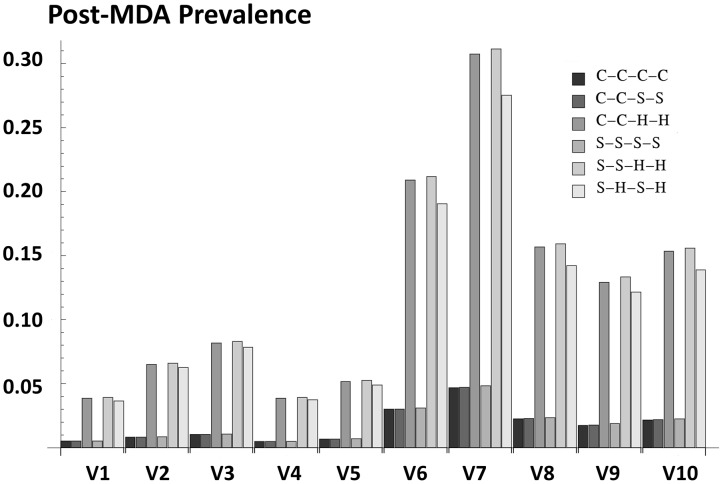
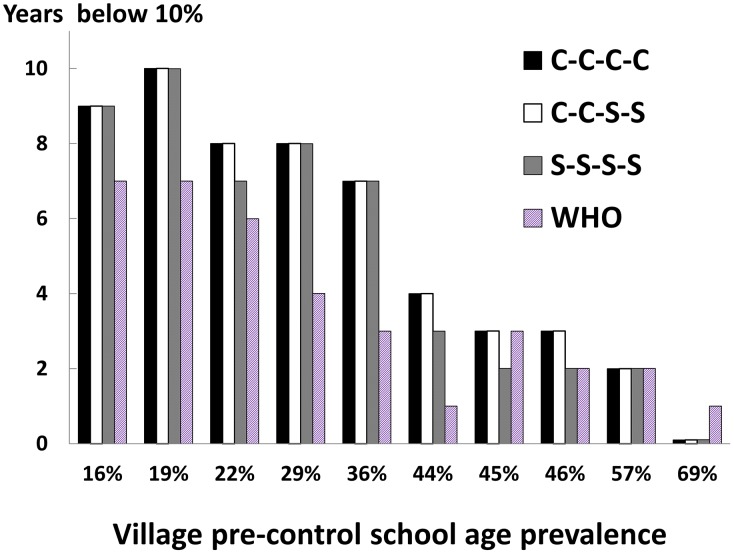
Methodology/principal findings: Our study used available field data to calibrate advanced network models of village-level Schistosoma transmission to project outcomes of six different community- or school age-based programs, as compared to the impact of current 2006 W.H.O. recommended control strategies. We then scored the number of years each of 10 typical villages would remain below 10% infection prevalence (a practicable level associated with minimal prevalence of disease). All strategies that included four annual treatments effectively reduced community prevalence to less than 10%, while programs having yearly gaps ('holidays') failed to reach this objective in half of the communities. Effective post-program suppression of infection prevalence persisted in half of the 10 villages for 7-10 years, whereas in five high-risk villages, program effects on prevalence lasted zero to four years only.
Conclusions/significance: At typical levels of treatment adherence (60 to 70%), current WHO recommendations will likely not achieve effective suppression of Schistosoma prevalence unless implemented for ≥6 years. Following more aggressive 4 year annual intervention, some communities may be able to continue without further intervention for 8-10 years, while in higher-risk communities, annual treatment may prove necessary until eco-social factors fostering transmission are removed. Effective ongoing surveillance and locally targeted annual intervention must then become their mainstays of control.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- WHO Expert Committee (2004) The World Health Report 2004-Changing History. Geneva: World Health Organization. 96 p.
-
- Hotez PJ, Molyneux DH, Fenwick A, Ottesen E, Sachs SE, et al. (2006) Incorporating a rapid-impact package for neglected tropical diseases with programs for HIV/AIDS, tuberculosis, and malaria - A comprehensive pro-poor health policy and strategy for the developing world. Plos Medicine 3: 576–584. - PMC - PubMed
-
- Jordan P (1985) Schistosomiasis: The St. Lucia Project. Cambridge: Cambridge University Press.
-
- Utzinger J, Zhou XN, Chen MG, Bergquist R (2005) Conquering schistosomiasis in China: the long march. Acta Trop 96: 69–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
