

Overuse of computed tomography pulmonary angiography in the evaluation of patients with suspected pulmonary embolism in the emergency department
- PMID: 23167851
- PMCID: PMC3506180
- DOI: 10.1111/acem.12012
Overuse of computed tomography pulmonary angiography in the evaluation of patients with suspected pulmonary embolism in the emergency department
Abstract
Background: Clinical decision rules have been developed and validated for the evaluation of patients presenting with suspected pulmonary embolism (PE) to the emergency department (ED).
Objectives: The objective was to assess the percentage of computed tomographic pulmonary angiography (CT-PA) procedures that could have been avoided by use of the Wells score coupled with D-dimer testing (Wells/D-dimer) or pulmonary embolism rule-out criteria (PERC) in ED patients with suspected PE.
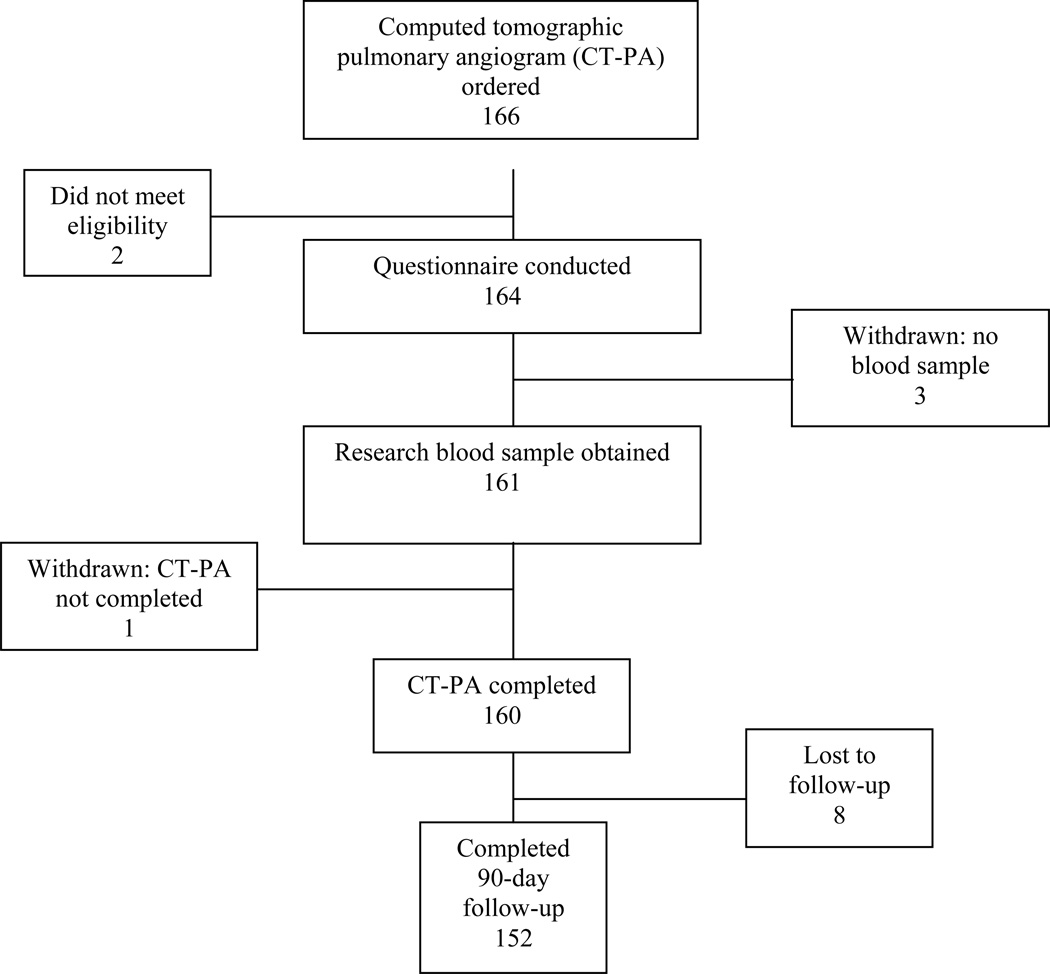
Methods: The authors conducted a prospective cohort study of adult ED patients undergoing CT-PA for suspected PE. Wells score and PERC were calculated. A research blood sample was obtained for D-dimer testing for subjects who did not undergo testing as part of their ED evaluation. The primary outcome was PE by CT-PA or 90-day follow-up. Secondary outcomes were ED length of stay (LOS) and CT-PA time as defined by time from order to initial radiologist interpretation.
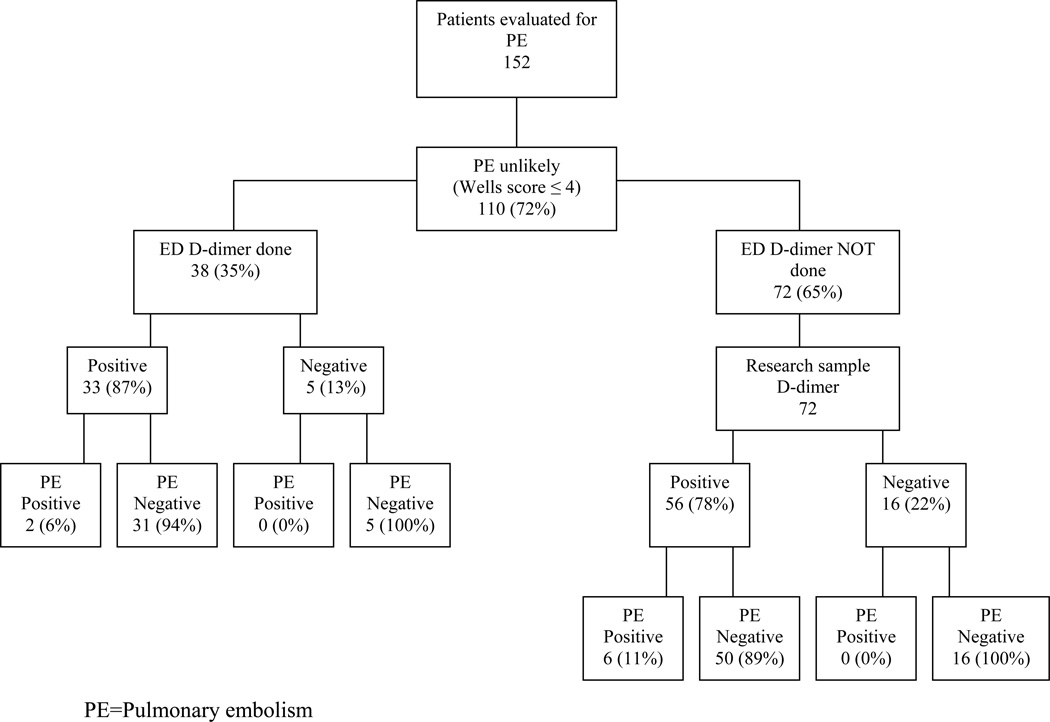
Results: Of 152 suspected PE subjects available for analysis (mean ± SD age = 46.3 ± 15.6 years, 74% female, 59% black or African American, 11.8% diagnosed with PE), 14 (9.2%) met PERC, none of whom were diagnosed with PE. A low-risk Wells score (≤4) was assigned to 110 (72%) subjects, of whom only 38 (35%) underwent clinical D-dimer testing (elevated in 33/38). Of the 72 subjects with low-risk Wells scores who did not have D-dimers performed in the ED, archived research samples were negative in 16 (22%). All 21 subjects with low-risk Wells scores and negative D-dimers were PE-negative. CT-PA time (median = 160 minutes) accounted for more than half of total ED LOS (median = 295 minutes).
Conclusions: In total, 9.2 and 13.8% of CT-PA procedures could have been avoided by use of PERC and Wells/D-dimer, respectively.
© 2012 by the Society for Academic Emergency Medicine.
Conflict of interest statement
The authors have no conflicts of interest for further funding disclosures to report.
Figures
References
-
- Kline JA, Courtney DM, Kabrhel C, et al. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. J Thromb Haemost. 2008;6(5):772–780. - PubMed
-
- Wells PS, Anderson DR, Rodger M, et al. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001;135(2):98–107. - PubMed
-
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost. 2000;83(3):416–420. - PubMed
-
- Runyon MS, Richman PB, Kline JA. Emergency medicine practitioner knowledge and use of decision rules for the evaluation of patients with suspected pulmonary embolism: variations by practice setting and training level. Acad Emerg Med. 2007;14(1):53–57. - PubMed
-
- Wolf SJ, McCubbin TR, Nordenholz KE, Naviaux NW, Haukoos JS. Assessment of the pulmonary embolism rule-out criteria rule for evaluation of suspected pulmonary embolism in the emergency department. Am J Emerg Med. 2008;26(2):181–185. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
