

Hyperlactatemia affects the association of hyperglycemia with mortality in nondiabetic adults with sepsis
- PMID: 23167858
- PMCID: PMC3506124
- DOI: 10.1111/acem.12015
Hyperlactatemia affects the association of hyperglycemia with mortality in nondiabetic adults with sepsis
Abstract
Background: Admission hyperglycemia has been reported as a mortality risk factor for septic nondiabetic patients; however, hyperglycemia's known association with hyperlactatemia was not addressed in these analyses.
Objectives: The objective was to determine whether the association of hyperglycemia with mortality remains significant when adjusted for concurrent hyperlactatemia.
Methods: This was a post hoc, nested analysis of a retrospective cohort study performed at a single center. Providers had identified study subjects during their emergency department (ED) encounters; all data were collected from the electronic medical record (EMR). Nondiabetic adult ED patients hospitalized for suspected infection, two or more systemic inflammatory response syndrome (SIRS) criteria, and simultaneous lactate and glucose testing in the ED were enrolled. The setting was the ED of an urban teaching hospital from 2007 to 2009. To evaluate the association of hyperglycemia (glucose > 200 mg/dL) with hyperlactatemia (lactate ≥ 4.0 mmol/L), a logistic regression model was created. The outcome was a diagnosis of hyperlactatemia, and the primary variable of interest was hyperglycemia. A second model was created to determine if coexisting hyperlactatemia affects hyperglycemia's association with mortality; the main outcome was 28-day mortality, and the primary risk variable was hyperglycemia with an interaction term for simultaneous hyperlactatemia. Both models were adjusted for demographics; comorbidities; presenting infectious source; and objective evidence of renal, respiratory, hematologic, or cardiovascular dysfunction.
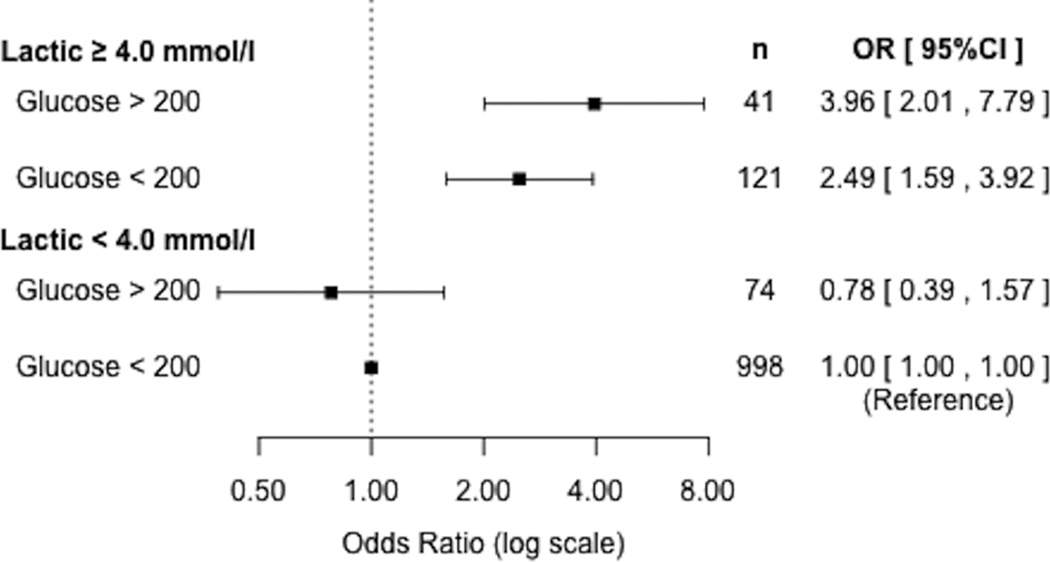
Results: A total of 1,236 ED patients were included, and the median age was 77 years (interquartile range [IQR] = 60 to 87 years). A total of 115 (9.3%) subjects were hyperglycemic, 162 (13%) were hyperlactatemic, and 214 (17%) died within 28 days of their initial ED visits. After adjustment, hyperglycemia was significantly associated with simultaneous hyperlactatemia (odds ratio [OR] = 4.14, 95% confidence interval [CI] = 2.65 to 6.45). Hyperglycemia and concurrent hyperlactatemia were associated with increased mortality risk (OR = 3.96, 95% CI = 2.01 to 7.79), but hyperglycemia in the absence of simultaneous hyperlactatemia was not (OR = 0.78, 95% CI = 0.39 to 1.57).
Conclusions: In this cohort of septic adult nondiabetic patients, mortality risk did not increase with hyperglycemia unless associated with simultaneous hyperlactatemia. The previously reported association of hyperglycemia with mortality in nondiabetic sepsis may be due to the association of hyperglycemia with hyperlactatemia.
© 2012 by the Society for Academic Emergency Medicine.
Figures
Similar articles
-
Impact of metformin use on the prognostic value of lactate in sepsis.Am J Emerg Med. 2012 Nov;30(9):1667-73. doi: 10.1016/j.ajem.2012.01.014. Epub 2012 Mar 16. Am J Emerg Med. 2012. PMID: 22424991 Free PMC article.
-
The utility of early lactate testing in undifferentiated pediatric systemic inflammatory response syndrome.Acad Emerg Med. 2012 Nov;19(11):1276-80. doi: 10.1111/acem.12014. Acad Emerg Med. 2012. PMID: 23167859
-
Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock.Crit Care Med. 2009 May;37(5):1670-7. doi: 10.1097/CCM.0b013e31819fcf68. Crit Care Med. 2009. PMID: 19325467
-
Risk Factors for Adverse Outcomes in Adult and Pediatric Patients With Hyperglycemia Presenting to the Emergency Department: A Systematic Review.Can J Diabetes. 2019 Jul;43(5):361-369.e2. doi: 10.1016/j.jcjd.2018.11.008. Epub 2018 Dec 6. Can J Diabetes. 2019. PMID: 30846250
-
Emergency Department Management of Uncomplicated Hyperglycemia in Patients without History of Diabetes.J Emerg Med. 2023 Aug;65(2):e81-e92. doi: 10.1016/j.jemermed.2023.04.018. Epub 2023 Apr 26. J Emerg Med. 2023. PMID: 37474343 Review.
Cited by
-
Influence of endocrine disease on l-lactate concentrations in blood of ponies.J Vet Intern Med. 2021 May;35(3):1582-1588. doi: 10.1111/jvim.16079. Epub 2021 May 27. J Vet Intern Med. 2021. PMID: 34043845 Free PMC article.
-
Glucose control in critical care.World J Diabetes. 2015 Aug 10;6(9):1082-91. doi: 10.4239/wjd.v6.i9.1082. World J Diabetes. 2015. PMID: 26265994 Free PMC article.
-
The association between stress hyperglycemia and poor outcome in critically ill children is modulated by hyperlactatemia.Front Endocrinol (Lausanne). 2025 Jun 18;16:1518746. doi: 10.3389/fendo.2025.1518746. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40607229 Free PMC article.
-
Intensive insulin therapy in sepsis patients: Better data enables better intervention.Heliyon. 2023 Feb 24;9(3):e14063. doi: 10.1016/j.heliyon.2023.e14063. eCollection 2023 Mar. Heliyon. 2023. PMID: 36915524 Free PMC article. Review.
-
Clinical and laboratory factors associated with neonatal sepsis mortality at a major Vietnamese children's hospital.PLOS Glob Public Health. 2022 Sep 2;2(9):e0000875. doi: 10.1371/journal.pgph.0000875. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962870 Free PMC article.
References
-
- Lagu T, Rothberg MB, Shieh MS, Pekow PS, Steingrub JS, Lindenauer PK. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012;40:754–761. - PubMed
-
- Gaieski DF, Mikkelsen ME, Band RA, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med. 2010;38:1045–1053. - PubMed
-
- Kumar A, Haery C, Paladugu B, et al. The duration of hypotension before the initiation of antibiotic treatment is a critical determinant of survival in a murine model of Escherichia coli septic shock: association with serum lactate and inflammatory cytokine levels. J Infect Dis. 2006;193:251–258. - PubMed
-
- Stegenga ME, Vincent JL, Vail GM, et al. Diabetes does not alter mortality or hemostatic and inflammatory responses in patients with severe sepsis. Crit Care Med. 2010;38:539–545. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
