

doi: 10.1186/1749-8090-7-125.
How I do it--sole innominate cannulation for acute type A aortic dissection
Affiliations
- PMID: 23167966
- PMCID: PMC3618214
- DOI: 10.1186/1749-8090-7-125
Item in Clipboard
How I do it--sole innominate cannulation for acute type A aortic dissection
J Cardiothorac Surg.
.
Abstract
We describe sole direct innominate cannulation for arterial return for establishing both cardiopulmonary bypass and selective antegrade cerebral perfusion in the repair of acute type A dissection and compare it with femoral, axillary, direct aortic and apical cannulations. We believe innominate cannulation has all the advantages of right axillary cannulation and none of its disadvantages. It can be used in all patients in whom innominate artery is not dissected, obstructed, calcified or otherwise diseased.
Figures
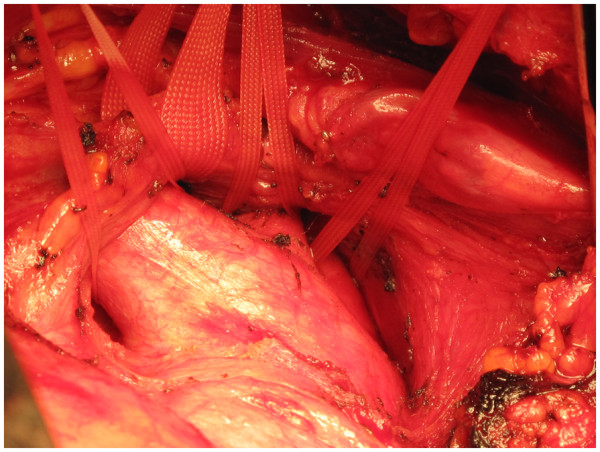
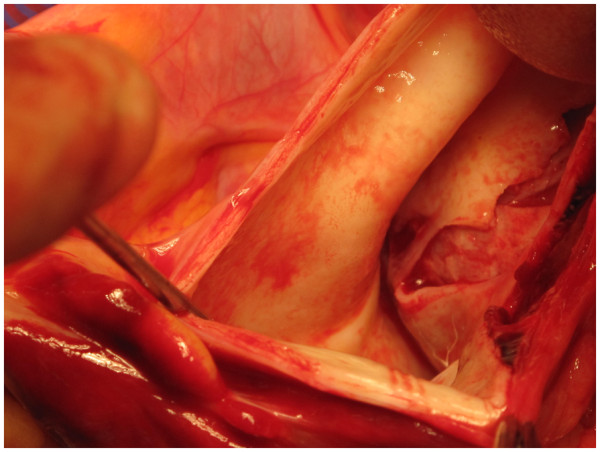
The left innominate vein (LIV), the innominate artery (IA), the left common carotid artery (LCCA) and the left subclavian artery (LSA) have been dissected and taped in a patient with type A dissection of aorta with a pre-existing aneurysm of aortic root and ascending aorta, before pericardium is opened.

A 20 F wire reinforced Medtronic cannula.
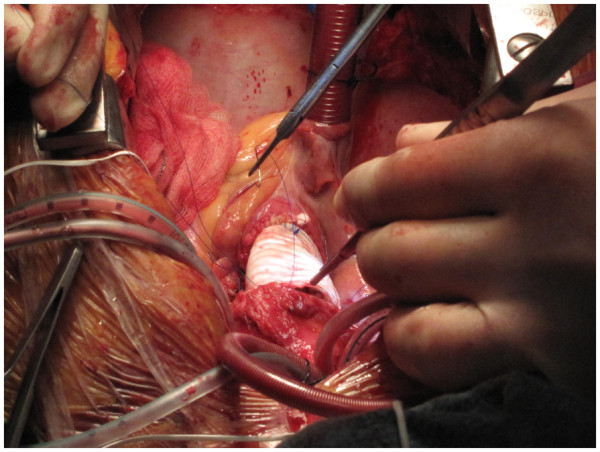
The innominate artery (IA) has been cannulated with 20 F Medtronic cannula which has been advanced into the arch.
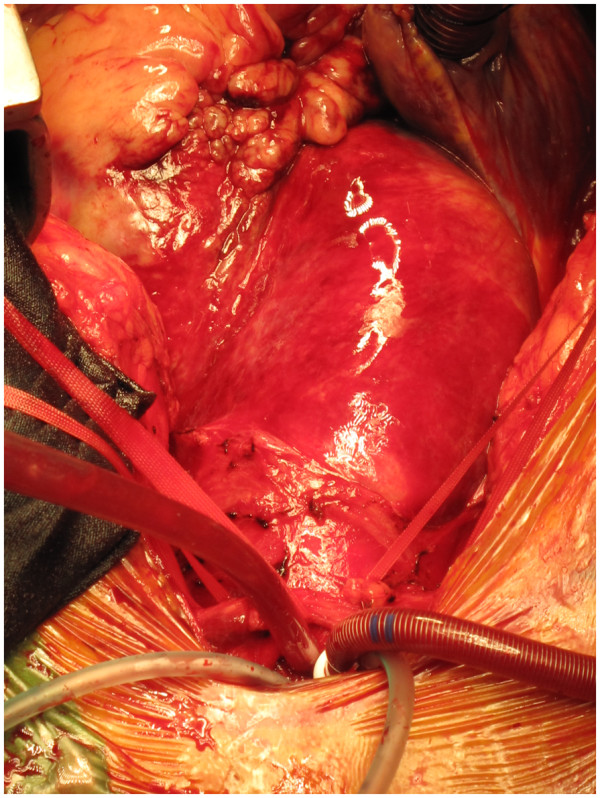
Pericardium is opened in a patient with type A dissection of aorta and as feared the aorta has ruptured with hemopericardium, but innominate artery (IA) is ready for cannulation and establishment of cardiopulmonary bypass.
The dissected aorta is cross clamped midway between the sinotubular junction and innominate artery origin at a place which will be subsequently excised. This does not pressurise the false lumen owing to antegrade flow in the arch through the innominate cannula.
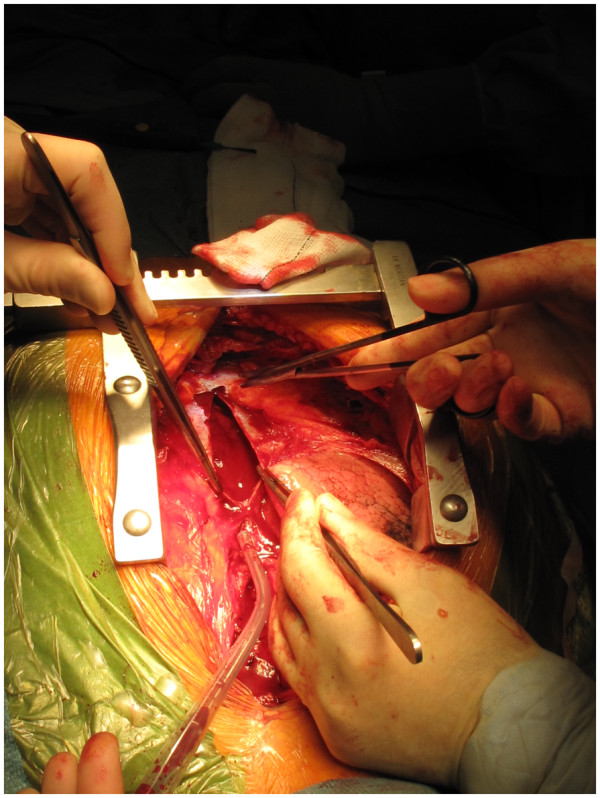
Long intimal tear in ascending aorta extending to just below the innominate artery. Whole of ascending aorta and whole of intimal tear must be excised in repair of type A dissection.
Retrograde dissection of ascending aorta from descending aortic intimal tear with pre-existing coronary artery disease. Repair included supra-coronary replacement of ascending aorta, suture repair of descending aortic tear and CABG X 3.
Open distal anastomosis with lower body circulatory arrest (LBCA) at 17 C and unihemispherical antegrade selective cerebral perfusion (ASCP) through the innominate cannula which has been redirected cranially. Decision for unihemispherical ASCP guided by adequate bilateral radial pressures, cerebral oxymetry and copious backflows from LCCA and LSA.
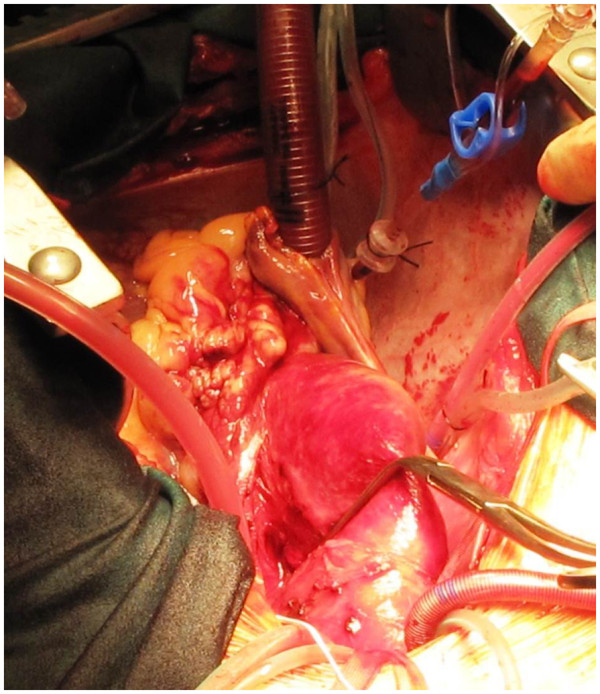
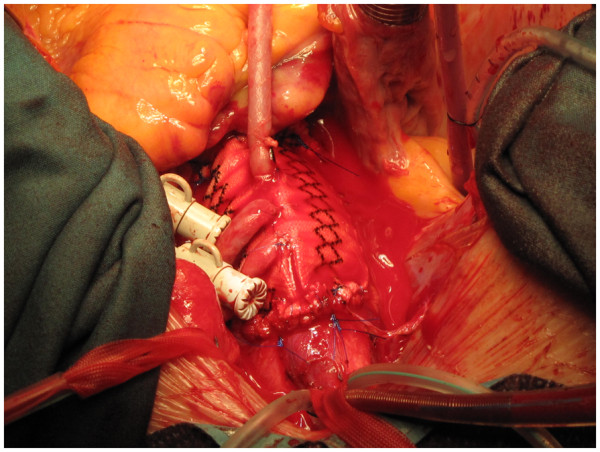
The completed dissection repair, the arch vessel tapes have been unsnugged and the innominate cannula redirected into the arch again.
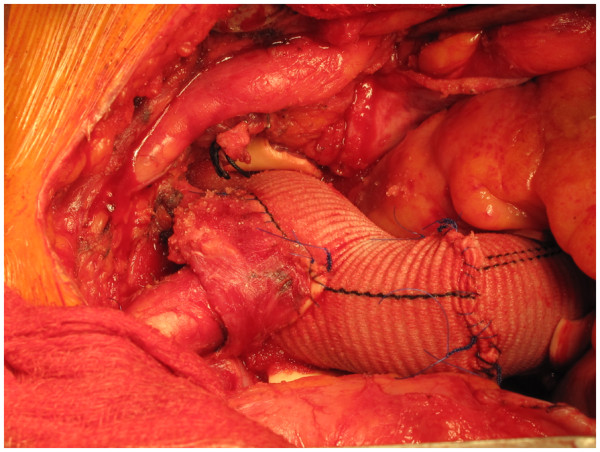
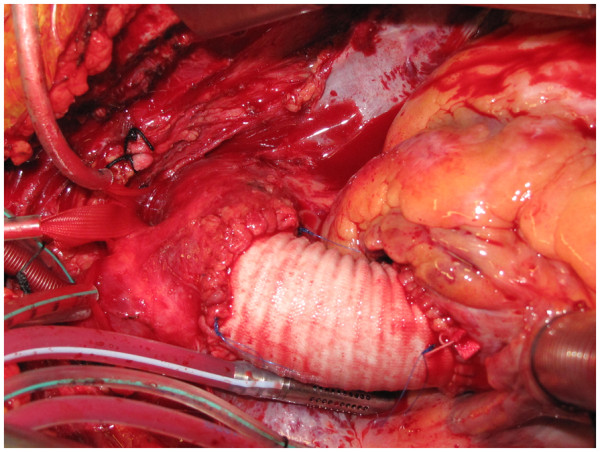
Aortic root, ascending aorta and total arch replacement in a patient with aneurysmal disease using composite innominate cannulation.
Similar articles
-
Is right axillary artery cannulation safe in type A aortic dissection with involvement of the innominate artery?J Thorac Cardiovasc Surg. 2016 Sep;152(3):801-807.e1. doi: 10.1016/j.jtcvs.2016.04.092. Epub 2016 May 10. J Thorac Cardiovasc Surg. 2016. PMID: 27239008
-
The use of innominate artery cannulation for antegrade cerebral perfusion in aortic dissection.J Cardiothorac Surg. 2020 Jul 31;15(1):205. doi: 10.1186/s13019-020-01249-1. J Cardiothorac Surg. 2020. PMID: 32736644 Free PMC article.
-
Direct Innominate Artery Cannulation as a Sole Systemic and Cerebral Perfusion Technique in Aortic Surgery.Heart Lung Circ. 2019 Apr;28(4):e67-e70. doi: 10.1016/j.hlc.2018.08.001. Epub 2018 Aug 28. Heart Lung Circ. 2019. PMID: 30269872
-
Does the arterial cannulation site for circulatory arrest influence stroke risk?Ann Thorac Surg. 2004 Oct;78(4):1274-84; discussion 1274-84. doi: 10.1016/j.athoracsur.2004.04.063. Ann Thorac Surg. 2004. PMID: 15464485 Review.
-
sArterial cannulation to establish cardiopulmonary bypass during surgery for acute aortic dissection.Surg Today. 2020 Nov;50(11):1353-1359. doi: 10.1007/s00595-019-01921-7. Epub 2019 Nov 26. Surg Today. 2020. PMID: 31773278 Review.
Cited by
-
Optimizing aortic arch branch cannulation in acute type A dissection surgery: a minimally invasive approach.Front Cardiovasc Med. 2025 May 16;12:1549736. doi: 10.3389/fcvm.2025.1549736. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40454235 Free PMC article.
-
Innominate truncal and arch blowout with left hemiparesis and right hemothorax followed by delayed cheese-wire perforation of innominate graft.J Cardiothorac Surg. 2013 Apr 23;8:109. doi: 10.1186/1749-8090-8-109. J Cardiothorac Surg. 2013. PMID: 23618057 Free PMC article.
-
Systematic Innominate Artery Cannulation Strategy in Acute Type A Aortic Dissection: Better Perfusion, Better Results.J Clin Med. 2023 Apr 13;12(8):2851. doi: 10.3390/jcm12082851. J Clin Med. 2023. PMID: 37109188 Free PMC article.
-
Sequential ruptures of penetrating atherosclerotic ulcers of ascending aorta, aortic arch and descending thoracic aorta.J Cardiothorac Surg. 2020 Oct 6;15(1):298. doi: 10.1186/s13019-020-01311-y. J Cardiothorac Surg. 2020. PMID: 33023614 Free PMC article.
References
-
- Baue AE. Glenn’s thoracic and cardiovascular surgery. 6th edn vol 2. Stanford, CT: Appleton and Lange; 1996. Dissections of the aorta; pp. 2273–2274.
-
- Debakey ME, McCollum CH, Crawford ES. Dissection and dissecting aneurysms of aorta: twenty year follow up of five hundred and twenty seven patients treated surgically. Surgery. 1982;92:1118–1134. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
