

The use of typing methods and infection prevention measures to control a bullous impetigo outbreak on a neonatal ward
- PMID: 23168170
- PMCID: PMC3546034
- DOI: 10.1186/2047-2994-1-37
The use of typing methods and infection prevention measures to control a bullous impetigo outbreak on a neonatal ward
Abstract
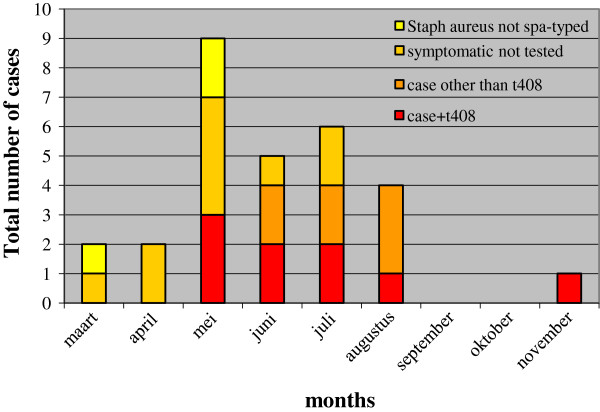
Background: We describe an outbreak of Bullous Impetigo (BI), caused by a (methicillin susceptible, fusidic acid resistant) Staphylococcus aureus (SA) strain, spa-type t408, at the neonatal and gynaecology ward of the Jeroen Bosch hospital in the Netherlands, from March-November 2011.
Methods: We performed an outbreak investigation with revision of the hygienic protocols, MSSA colonization surveillance and environmental sampling for MSSA including detailed typing of SA isolates. Spa typing was performed to discriminate between the SA isolates. In addition, Raman-typing was performed on all t408 isolates.
Results: Nineteen cases of BI were confirmed by SA positive cultures. A cluster of nine neonates and three health care workers (HCW) with SA t408 was detected. These strains were MecA-, PVL-, Exfoliative Toxin (ET)A-, ETB+, ETAD-, fusidic acid-resistant and methicillin susceptible. Eight out of nine neonates and two out of three HCW t408 strains yielded a similar Raman type. Positive t408 HCW were treated and infection control procedures were reinforced. These measures stopped the outbreak.
Conclusions: We conclude that treatment of patients and HCW carrying a predominant SA t408, and re-implementing and emphasising hygienic measures were effective to control the outbreak of SA t408 among neonates.
Figures
Similar articles
-
Next-Generation Sequence Analysis Reveals Transfer of Methicillin Resistance to a Methicillin-Susceptible Staphylococcus aureus Strain That Subsequently Caused a Methicillin-Resistant Staphylococcus aureus Outbreak: a Descriptive Study.J Clin Microbiol. 2017 Sep;55(9):2808-2816. doi: 10.1128/JCM.00459-17. Epub 2017 Jul 5. J Clin Microbiol. 2017. PMID: 28679522 Free PMC article.
-
Outbreak of bullous impetigo caused by Staphylococcus aureus strains of phage type 3C/71 in a maternity ward linked to nasal carriage of a healthcare worker.Eur J Dermatol. 2012 Mar-Apr;22(2):252-5. doi: 10.1684/ejd.2012.1671. Eur J Dermatol. 2012. PMID: 22378195
-
Outbreak of methicillin-resistant Staphylococcus aureus colonization and infection in a neonatal intensive care unit epidemiologically linked to a healthcare worker with chronic otitis.Infect Control Hosp Epidemiol. 2006 Jun;27(6):581-5. doi: 10.1086/504933. Epub 2006 May 25. Infect Control Hosp Epidemiol. 2006. PMID: 16755477
-
Molecular typing of toxic shock syndrome toxin-1- and Enterotoxin A-producing methicillin-sensitive Staphylococcus aureus isolates from an outbreak in a neonatal intensive care unit.Int J Med Microbiol. 2015 Oct;305(7):790-8. doi: 10.1016/j.ijmm.2015.08.033. Epub 2015 Aug 22. Int J Med Microbiol. 2015. PMID: 26321006
-
Prolonged outbreak of Staphylococcus aureus surgical site infection traced to a healthcare worker with psoriasis.J Hosp Infect. 2014 Jan;86(1):42-6. doi: 10.1016/j.jhin.2013.10.006. Epub 2013 Oct 31. J Hosp Infect. 2014. PMID: 24296162
Cited by
-
Whole-genome sequencing to explore nosocomial transmission and virulence in neonatal methicillin-susceptible Staphylococcus aureus bacteremia.Antimicrob Resist Infect Control. 2020 Feb 22;9(1):39. doi: 10.1186/s13756-020-0699-8. Antimicrob Resist Infect Control. 2020. PMID: 32087747 Free PMC article.
-
An outbreak of skin infections in neonates due to a Staphylococcus aureus strain producing the exfoliative toxin A.Infection. 2018 Feb;46(1):49-54. doi: 10.1007/s15010-017-1084-2. Epub 2017 Nov 6. Infection. 2018. PMID: 29110142
References
-
- Koning S, Mohammedamin RSA, van der Wouden JC. et al.Impetigo: incidence and treatment in Dutch general practice in 1987 and 2001 - results from two national surveys. Br J Dermatol. 2005;154:239–242. - PubMed
LinkOut - more resources
Full Text Sources
