

Indexes of von Willebrand factor as biomarkers of aortic stenosis severity (from the Biomarkers of Aortic Stenosis Severity [BASS] study)
- PMID: 23168287
- PMCID: PMC3932487
- DOI: 10.1016/j.amjcard.2012.10.015
Indexes of von Willebrand factor as biomarkers of aortic stenosis severity (from the Biomarkers of Aortic Stenosis Severity [BASS] study)
Abstract
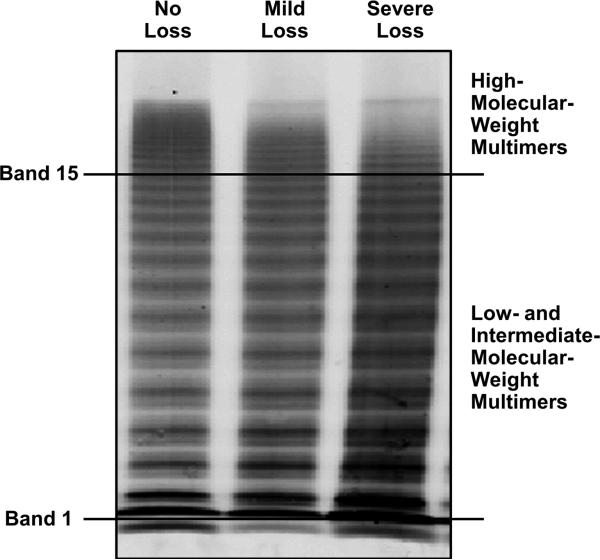
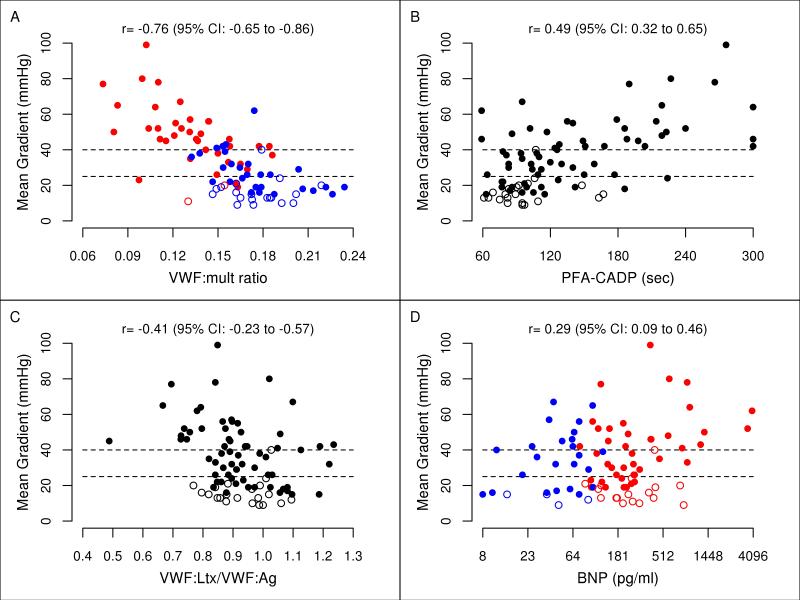
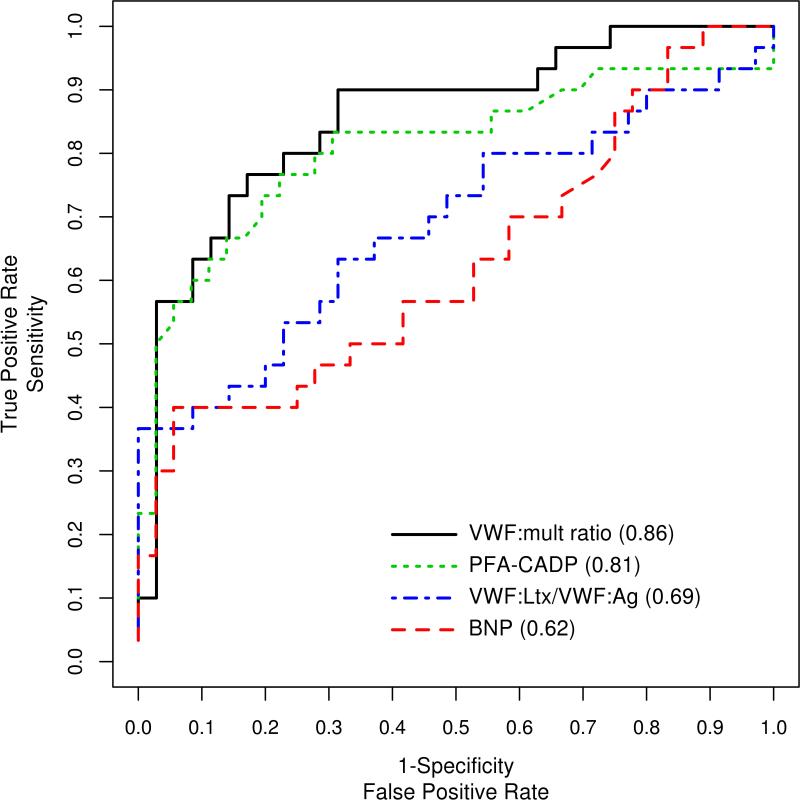
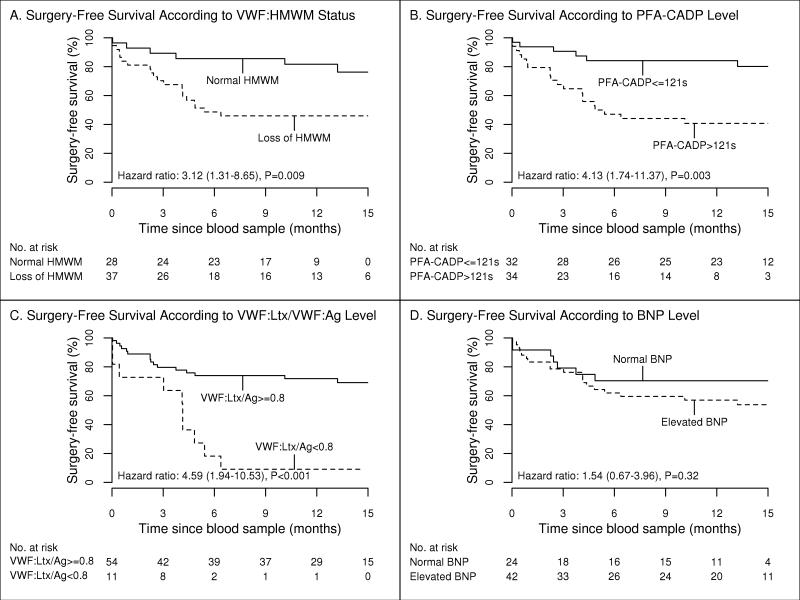
We correlated von Willebrand factor (VWF) activity indexes and brain natriuretic peptide (BNP) with measures of aortic stenosis (AS) severity, bleeding, symptoms, and freedom from death or aortic valve replacement. Patients with AS (n = 66 [16 mild, 20 moderate, and 30 severe]) and aortic valve replacement (n = 21) were assessed with VWF antigen, VWF latex agglutination immunoturbidic activity, platelet function analyzer collagen plus adenosine diphosphate (PFA-CADP), VWF multimer ratio, and BNP level after echocardiography. In patients with AS, the mean gradient correlated with BNP (Spearman r = 0.29, p = 0.02), VWF latex agglutination immunoturbidic activity/VWF antigen ratio (r = -0.41, p <0.001), PFA-CADP (r = 0.49, p <0.001), and VWF multimer ratio (r = -0.76, p <0.001). The area under the curve for detection of severe AS was 0.62 (95% confidence interval [CI] 0.48 to 0.77) by elevated BNP, 0.81 (95% CI 0.69 to 0.92) by PFA-CADP closure time, 0.69 (95% CI 0.55 to 0.82) by VWF latex agglutination immunoturbidic activity/VWF antigen ratio, and 0.86 (95% CI 0.76 to 0.95) by VWF multimer ratio. For the VWF multimer ratio, a threshold of 0.15 yielded a sensitivity and specificity for severe AS of 77% and positive predictive value of 74%. Bleeding (in 14%) was associated with a prolonged PFA-CADP time and reduced VWF latex agglutination immunoturbidic activity/VWF antigen ratio. Symptoms were associated with elevated BNP and low Duke Activity Status Index score. In 66 patients with AS, freedom from death (n = 4) or aortic valve replacement (n = 22) was associated with PFA-CADP (p = 0.003), VWF high-molecular-weight multimers (p = 0.009), and VWF latex agglutination immunoturbidic activity/VWF antigen ratio (p <0.001) but not BNP (p = 0.32). In severe AS versus aortic valve replacement, the PFA-CADP and VWF multimer ratio differed (p <0.001), but BNP and the VWF latex agglutination immunoturbidic activity/VWF antigen ratio did not. In conclusion, the VWF activity indexes were associated with AS severity and bleeding and were predictive of cardiovascular outcomes.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Baumgartner H, Stefenelli T, Niederberger J, Schima H, Maurer G. “Overestimation” of catheter gradients by Doppler ultrasound in patients with aortic stenosis: a predictable manifestation of pressure recovery. J Am Coll Cardiol. 1999;33:1655–1661. - PubMed
-
- Minners J, Allgeier M, Gohlke-Baerwolf C, Kienzle RP, Neumann FJ, Jander N. Inconsistencies of echocardiographic criteria for the grading of aortic valve stenosis. Eur Heart J. 2008;29:1043–1048. - PubMed
-
- Bahlmann E, Cramariuc D, Gerdts E, Gohlke-Baerwolf C, Nienaber CA, Eriksen E, Wachtell K, Chambers J, Kuck KH, Ray S. Impact of pressure recovery on echocardiographic assessment of asymptomatic aortic stenosis: a SEAS substudy. JACC Cardiovasc Imaging. 2010;3:555–562. - PubMed
-
- Kurtz CE, Otto CM. Aortic stenosis: clinical aspects of diagnosis and management, with 10 illustrative case reports from a 25-year experience. Medicine (Baltimore) 2010;89:349–379. - PubMed
-
- Vahanian A, Otto CM. Risk stratification of patients with aortic stenosis. Eur Heart J. 2010;31:416–423. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
