

General health checks in adults for reducing morbidity and mortality from disease: Cochrane systematic review and meta-analysis
- PMID: 23169868
- PMCID: PMC3502745
- DOI: 10.1136/bmj.e7191
General health checks in adults for reducing morbidity and mortality from disease: Cochrane systematic review and meta-analysis
Abstract
Objectives: To quantify the benefits and harms of general health checks in adults with an emphasis on patient-relevant outcomes such as morbidity and mortality rather than on surrogate outcomes.
Design: Cochrane systematic review and meta-analysis of randomised trials. For mortality, we analysed the results with random effects meta-analysis, and for other outcomes we did a qualitative synthesis as meta-analysis was not feasible.
Data sources: Medline, EMBASE, Healthstar, Cochrane Library, Cochrane Central Register of Controlled Trials, CINAHL, EPOC register, ClinicalTrials.gov, and WHO ICTRP, supplemented by manual searches of reference lists of included studies, citation tracking (Web of Knowledge), and contacts with trialists.
Selection criteria: Randomised trials comparing health checks with no health checks in adult populations unselected for disease or risk factors. Health checks defined as screening general populations for more than one disease or risk factor in more than one organ system. We did not include geriatric trials.
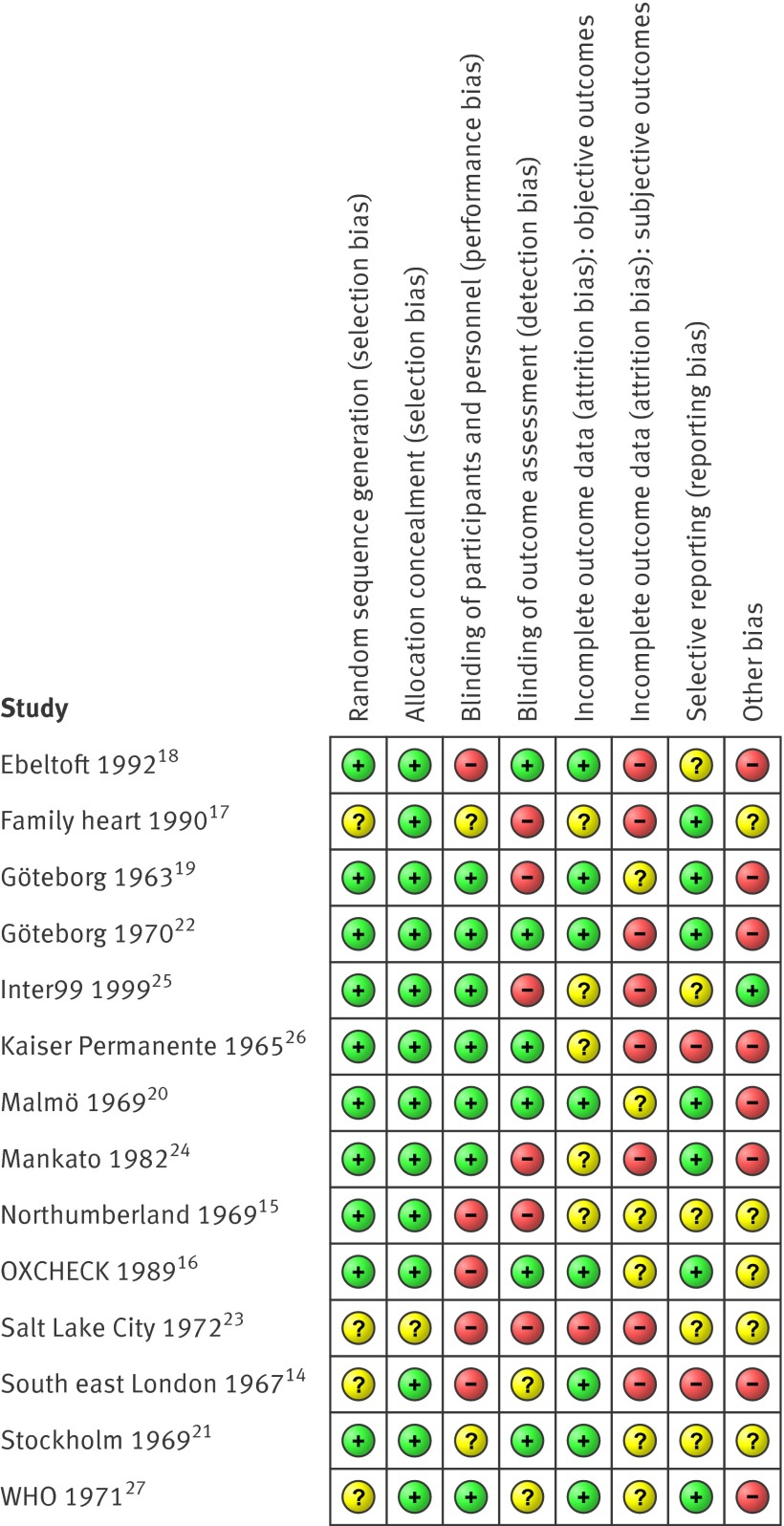
Data extraction: Two observers independently assessed eligibility, extracted data, and assessed the risk of bias. We contacted authors for additional outcomes or trial details when necessary.
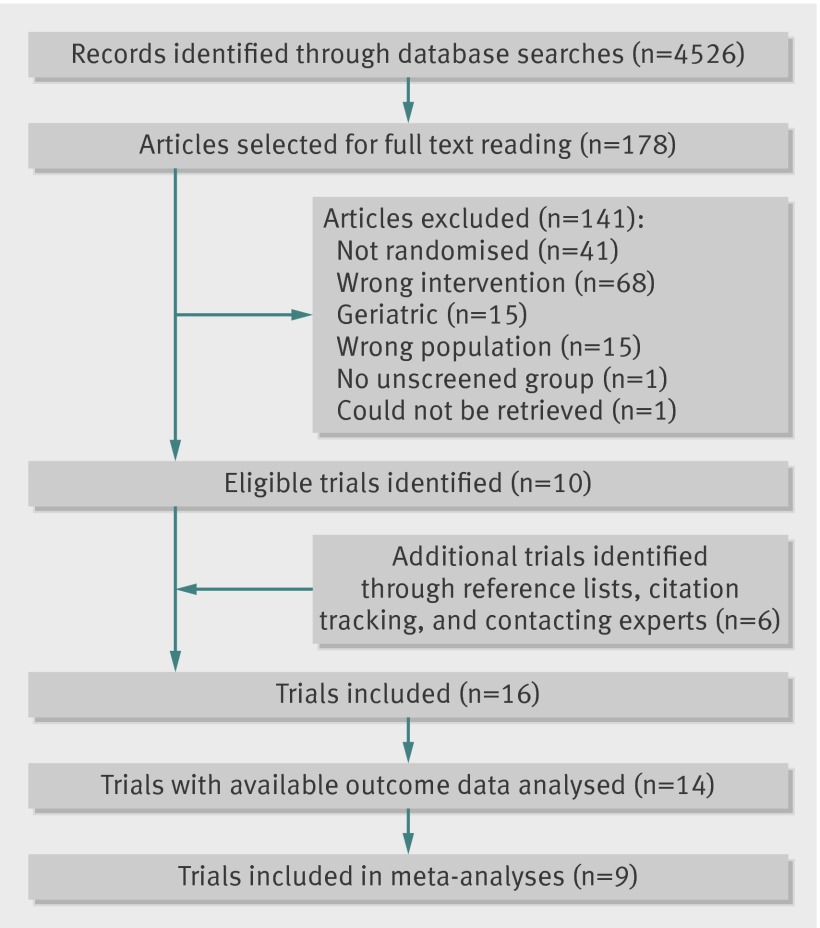
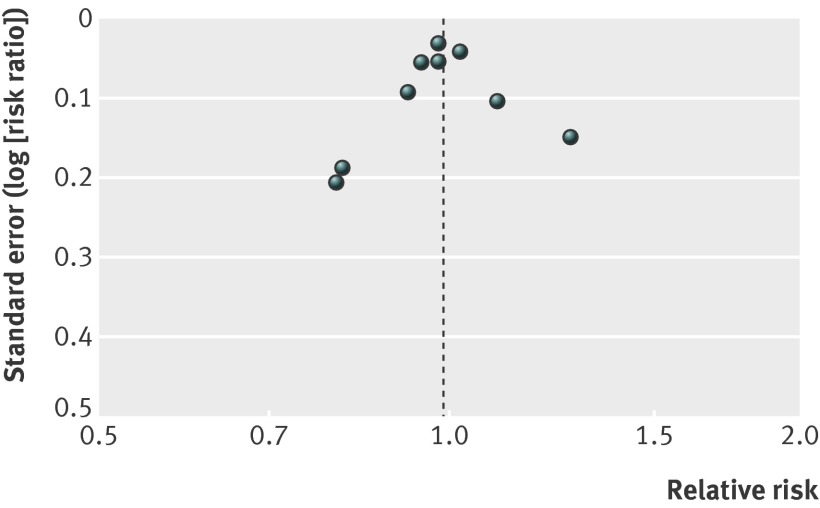
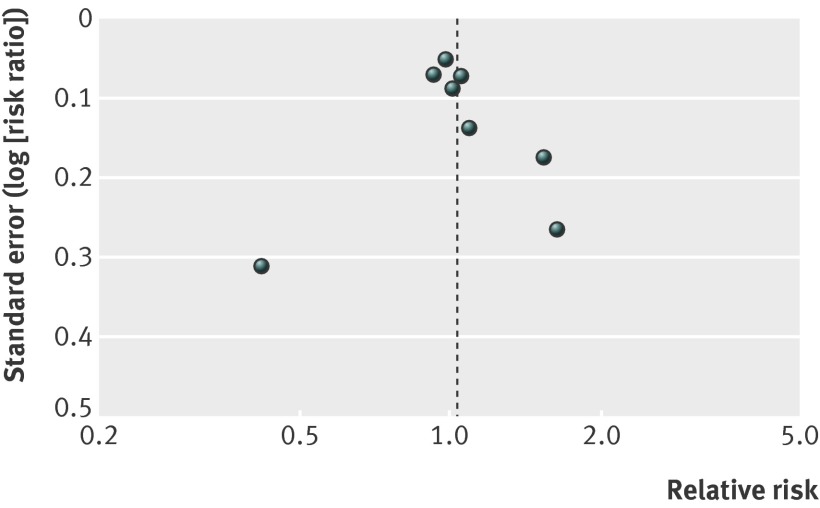
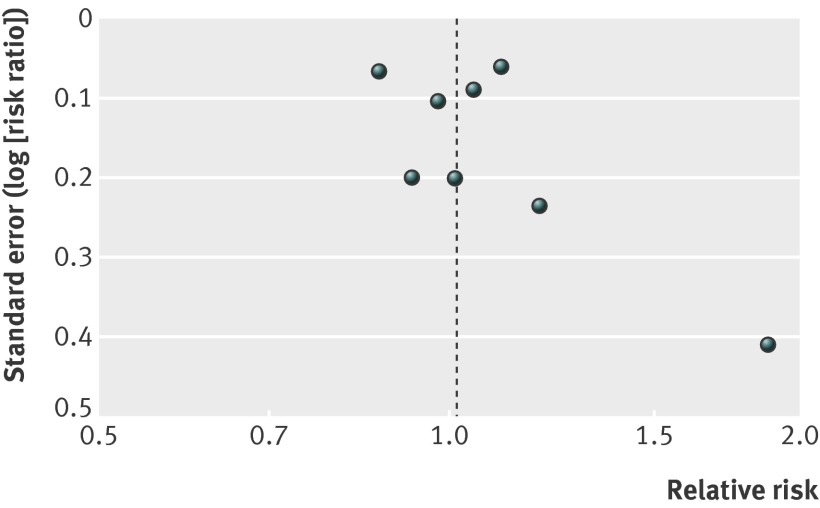
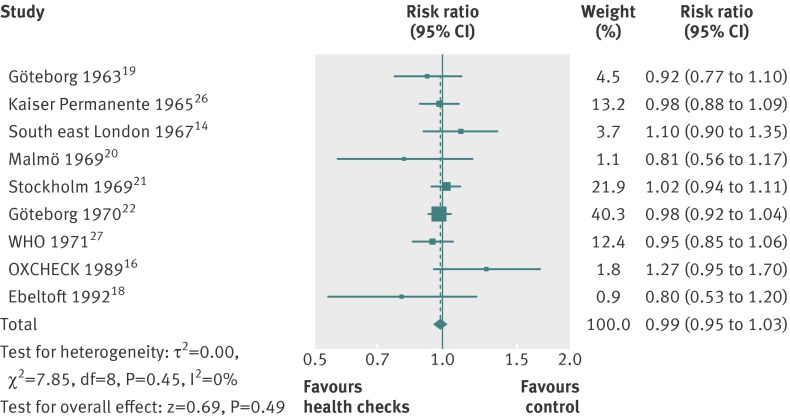
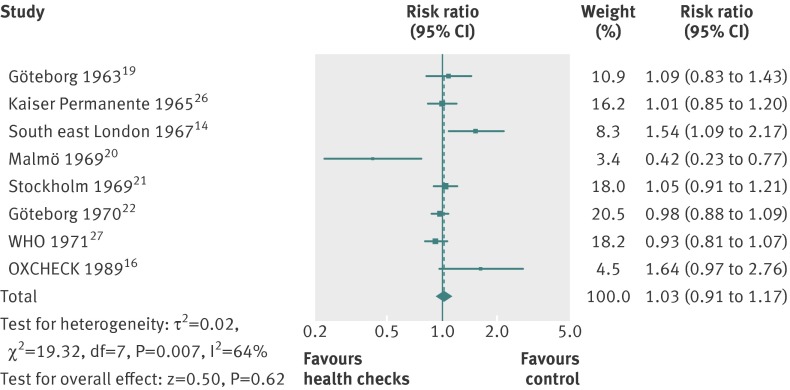
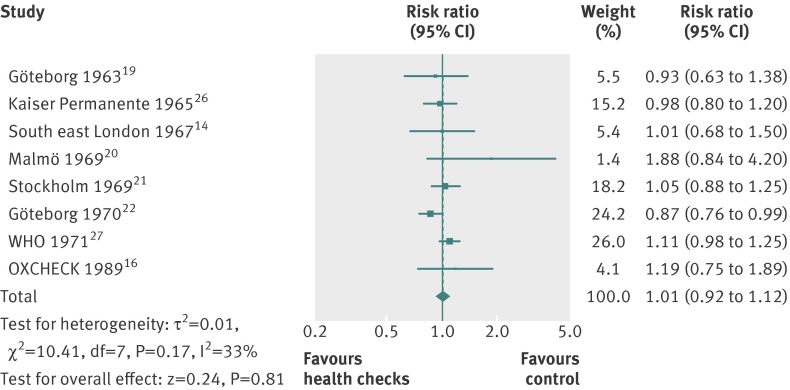
Results: We identified 16 trials, 14 of which had available outcome data (182,880 participants). Nine trials provided data on total mortality (11,940 deaths), and they gave a risk ratio of 0.99 (95% confidence interval 0.95 to 1.03). Eight trials provided data on cardiovascular mortality (4567 deaths), risk ratio 1.03 (0.91 to 1.17), and eight on cancer mortality (3663 deaths), risk ratio 1.01 (0.92 to 1.12). Subgroup and sensitivity analyses did not alter these findings. We did not find beneficial effects of general health checks on morbidity, hospitalisation, disability, worry, additional physician visits, or absence from work, but not all trials reported on these outcomes. One trial found that health checks led to a 20% increase in the total number of new diagnoses per participant over six years compared with the control group and an increased number of people with self reported chronic conditions, and one trial found an increased prevalence of hypertension and hypercholesterolaemia. Two out of four trials found an increased use of antihypertensives. Two out of four trials found small beneficial effects on self reported health, which could be due to bias.
Conclusions: General health checks did not reduce morbidity or mortality, neither overall nor for cardiovascular or cancer causes, although they increased the number of new diagnoses. Important harmful outcomes were often not studied or reported.
Systematic review registration: Cochrane Library, doi:10.1002/14651858.CD009009.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
The value of conducting periodic health checks.BMJ. 2012 Nov 20;345:e7775. doi: 10.1136/bmj.e7775. BMJ. 2012. PMID: 23169871 No abstract available.
References
-
- Han PKJ. Historical changes in the objectives of the periodic health examination. Ann Intern Med 1997;127:910-7. - PubMed
-
- Holland W. Periodic health examination—a brief history and critical assessment. Eurohealth 2009;15:16-20.
-
- Norris SL, Kansagara D, Bougatsos C, Fu R, for the US Preventive Services Task Force. Screening adults for type 2 diabetes: a review of the evidence for the US Preventive Services Task Force. Ann Intern Med 2008;148:855-68. - PubMed
-
- Sheridan S, Pignone M, Donahue K. Screening for high blood pressure: a review of the evidence for the US Preventive Services Task Force. Am J Prev Med 2003;25:151-8.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources