

High viremia and low level of transmitted drug resistance in anti-retroviral therapy-naïve perinatally-infected children and adolescents with HIV-1 subtype C infection
- PMID: 23171203
- PMCID: PMC3537751
- DOI: 10.1186/1471-2334-12-317
High viremia and low level of transmitted drug resistance in anti-retroviral therapy-naïve perinatally-infected children and adolescents with HIV-1 subtype C infection
Abstract
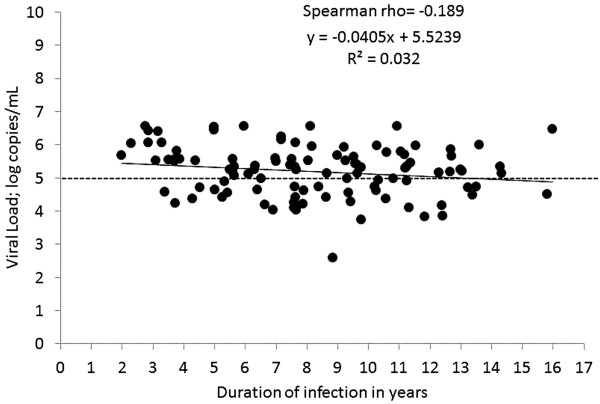
Background: High plasma viremia in HIV-1 infection is associated with rapid CD4 cell decline and faster disease progression. Children with HIV infection have high viral loads, particularly in early childhood. In this study we sought to understand the relationship between duration of HIV-1 infection and viral dynamics among perinatally-infected children and adolescents in India along with transmitted drug resistance in this population.
Methods: During 2007-2011, cross-sectional samples were collected from ART-naïve children (n = 105) with perinatally-acquired HIV infection, aged 2-16 years from Bangalore, India. CD4 counts, viral load and in-house genotyping were performed and transmitted drug resistance mutations were identified using the World Health Organization recommendations for Surveillance of Drug Resistance Mutations (SDRM_2009) list.
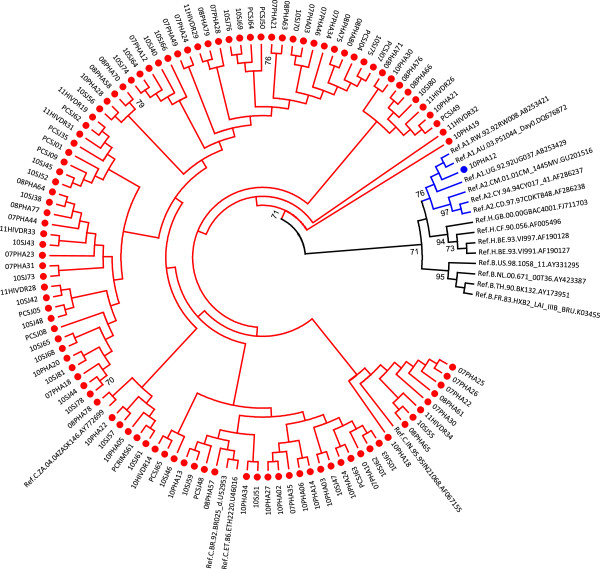
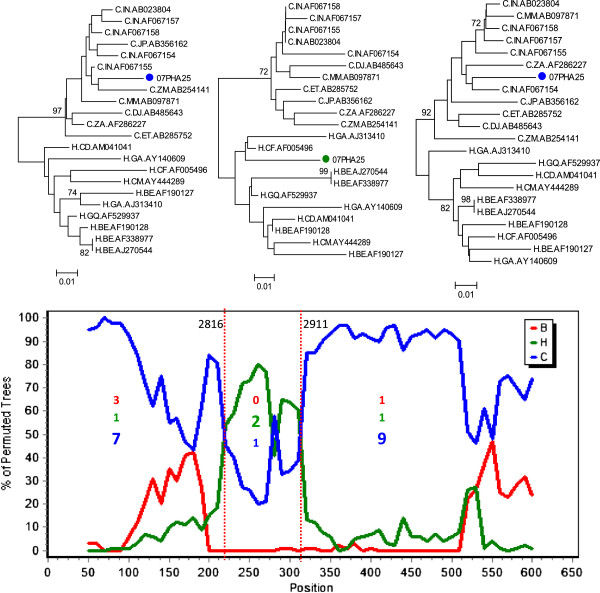
Results: Among 105 children studied, 73.3% (77/105) were asymptomatic, but had a median viral load of 5.24 log copies/mL (IQR 4.62-5.66). In the adolescent age group, 54% (21/39) had high levels of viremia (median 5.14 log copies/mL) but were asymptomatic. HIV-1 subtyping identified 98% strains (103/105) as subtype C; one A1 and one unique recombinant form (URF). Transmitted NRTI resistance was 1.9% (2/105); NNRTI resistance was 4.8% (5/105) and overall prevalence of transmitted drug resistance was 5.7% (6/105).
Conclusions: The high burden of plasma viremia found among untreated asymptomatic adolescents needs to be addressed both from an individual angle to halt disease progression, and from a public health perspective to arrest horizontal transmission. The low level of transmitted drug resistance among perinatally-infected children is reassuring; however with improving ART access globally, regular genotyping surveillance is indicated.
Figures
References
-
- National AIDS Control Organization, Annual Report, 2009–2010. http://nacoonline.org/upload/AR%202009-10/NACO_AR_English%20corrected.pdf.
-
- Shankarappa R, Margolick JB, Gange SJ, Rodrigo AG, Upchurch D, Farzadegan H, Gupta P, Rinaldo CR, Learn GH, He X, Huang XL, Mullins JI. Consistent viral evolutionary changes associated with the progression of human immunodeficiency virus type 1 infection. J Virol. 1999;73:10489–10502. - PMC - PubMed
-
- Shearer WT, Quinn TC, LaRussa P, Lew JF, Mofenson L, Almy S, Rich K, Handelsman E, Diaz C, Pagano M, Smeriglio V, Kalish LA. Viral load and disease progression in infants infected with human immunodeficiency virus type 1. Women and Infants Transmission Study Group. N Engl J Med. 1997;336:1337–1342. doi: 10.1056/NEJM199705083361901. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
