

Severe hyperkalemia requiring hospitalization: predictors of mortality
- PMID: 23171442
- PMCID: PMC3672605
- DOI: 10.1186/cc11872
Severe hyperkalemia requiring hospitalization: predictors of mortality
Abstract
Introduction: Severe hyperkalemia, with potassium (K+) levels ≥ 6.5 mEq/L, is a potentially life-threatening electrolyte imbalance. For prompt and effective treatment, it is important to know its risk factors, clinical manifestations, and predictors of mortality.
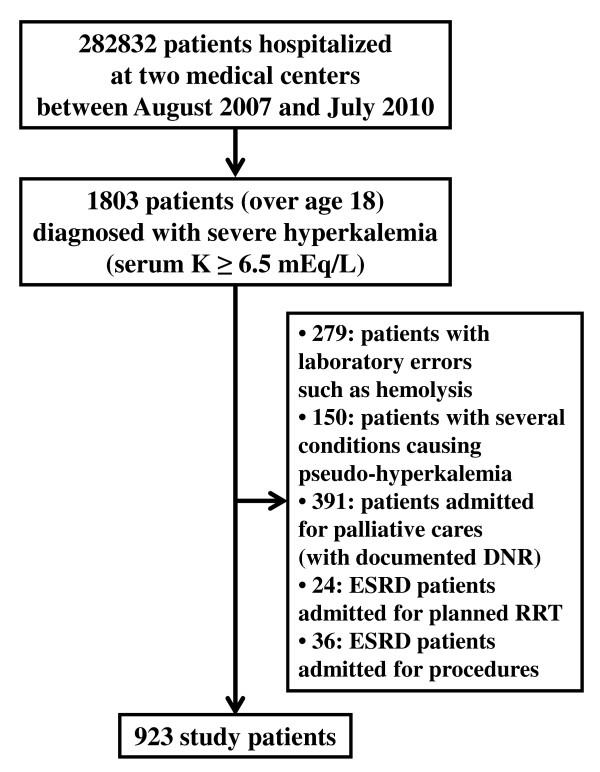
Methods: An observational cohort study was performed at 2 medical centers. A total of 923 consecutive Korean patients were analyzed. All were 19 years of age or older and were hospitalized with severe hyperkalemia between August 2007 and July 2010; the diagnosis of severe hyperkalemia was made either at the time of admission to the hospital or during the period of hospitalization. Demographic and baseline clinical characteristics at the time of hyperkalemia diagnosis were assessed, and clinical outcomes such as in-hospital mortality were reviewed, using the institutions' electronic medical record systems.
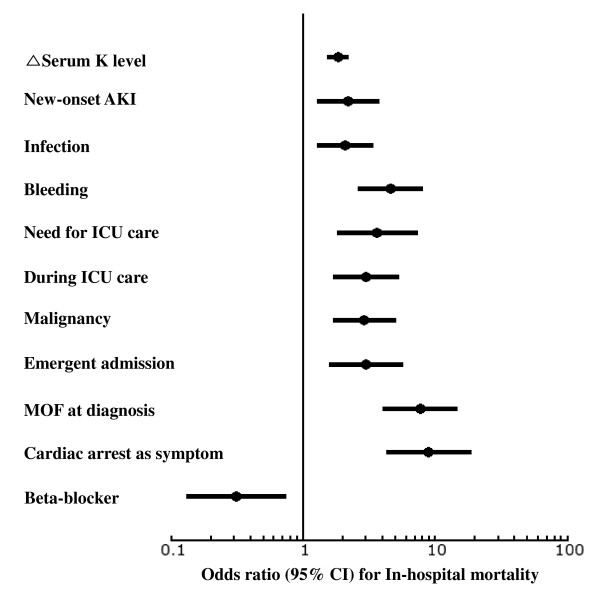
Results: Chronic kidney disease (CKD) was the most common underlying medical condition, and the most common precipitating factor of hyperkalemia was metabolic acidosis. Emergent admission was indicated in 68.6% of patients, 36.7% had electrocardiogram findings typical of hyperkalemia, 24.5% had multi-organ failure (MOF) at the time of hyperkalemia diagnosis, and 20.3% were diagnosed with severe hyperkalemia at the time of cardiac arrest. The in-hospital mortality rate was 30.7%; the rate was strongly correlated with the difference between serum K+ levels at admission and at their highest point, and with severe medical conditions such as malignancy, infection, and bleeding. Furthermore, a higher in-hospital mortality rate was significantly associated with the presence of cardiac arrest and/or MOF at the time of diagnosis, emergent admission, and intensive care unit treatment during hospitalization. More importantly, acute kidney injury (AKI) in patients with normal baseline renal function was a strong predictor of mortality, compared with AKI superimposed on CKD.
Conclusions: Severe hyperkalemia occurs in various medical conditions; the precipitating factors are similarly diverse. The mortality rate is especially high in patients with severe underlying disease, coexisting medical conditions, and those with normal baseline renal function.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
