

LHRH Agonists for the Treatment of Prostate Cancer: 2012
- PMID: 23172994
- PMCID: PMC3503273
LHRH Agonists for the Treatment of Prostate Cancer: 2012
Abstract
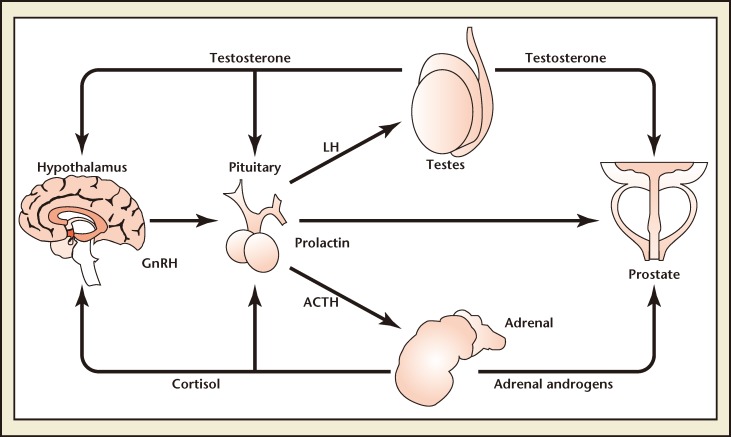
The most recent guidelines on prostate cancer screening from the American Urological Association (2009), the National Comprehensive Cancer Network (2011), and the European Association of Urology (2011), as well as treatment and advances in disease monitoring, have increased the androgen deprivation therapy (ADT) population and the duration of ADT usage as the first-line treatment for metastatic prostate cancer. According to the European Association of Urology, gonadotropin-releasing hormone (GnRH) agonists have become the leading therapeutic option for ADT because they avoid the physical and psychological discomforts associated with orchiectomy. However, GnRH agonists display several shortcomings, including testosterone (T) surge ("clinical flare") and microsurges. T surge delays the intended serologic endpoint of T suppression and may exacerbate clinical symptoms. Furthermore, ADT manifests an adverse-event spectrum that can impact quality of life with its attendant well-documented morbidities. Strategies to improve ADT tolerability include a holistic management approach, improved diet and exercise, and more specific monitoring to detect and prevent T depletion toxicities. Intermittent ADT, which allows hormonal recovery between treatment periods, has become increasingly utilized as a methodology for improving quality of life while not diminishing chronic ADT efficacy, and may also provide healthcare cost savings. This review assesses the present and potential future role of GnRH agonists in prostate cancer and explores strategies to minimize the adverse-event profile for patients receiving ADT.
Keywords: Androgen deprivation therapy; Gonadotropin-releasing hormone, agonists; Prostate cancer.
Figures
Similar articles
-
New considerations for ADT in advanced prostate cancer and the emerging role of GnRH antagonists.Prostate Cancer Prostatic Dis. 2013 Mar;16(1):7-15. doi: 10.1038/pcan.2012.25. Epub 2012 Jul 3. Prostate Cancer Prostatic Dis. 2013. PMID: 22751146 Review.
-
Relugolix: a novel androgen deprivation therapy for management of patients with advanced prostate cancer.Ther Adv Med Oncol. 2021 Mar 24;13:1758835921998586. doi: 10.1177/1758835921998586. eCollection 2021. Ther Adv Med Oncol. 2021. PMID: 34408793 Free PMC article. Review.
-
Bench-to-bedside development of agonists and antagonists of luteinizing hormone-releasing hormone for treatment of advanced prostate cancer.Urol Oncol. 2015 Jun;33(6):270-4. doi: 10.1016/j.urolonc.2014.11.006. Epub 2014 Dec 13. Urol Oncol. 2015. PMID: 25512159 Review.
-
An update on the use of gonadotropin-releasing hormone antagonists in prostate cancer.Ther Adv Urol. 2011 Jun;3(3):127-40. doi: 10.1177/1756287211414457. Ther Adv Urol. 2011. PMID: 21904569 Free PMC article.
-
An Expert Review on the Combination of Relugolix With Definitive Radiation Therapy for Prostate Cancer.Int J Radiat Oncol Biol Phys. 2022 Jun 1;113(2):278-289. doi: 10.1016/j.ijrobp.2021.12.005. Epub 2021 Dec 17. Int J Radiat Oncol Biol Phys. 2022. PMID: 34923058 Review.
Cited by
-
The Role of Androgen Receptor in Cross Talk Between Stromal Cells and Prostate Cancer Epithelial Cells.Front Cell Dev Biol. 2021 Oct 6;9:729498. doi: 10.3389/fcell.2021.729498. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34692685 Free PMC article. Review.
-
The presence of a pituitary tumor in patients with prostate cancer is not a contraindication for leuprolide therapy.Int Urol Nephrol. 2014 Sep;46(9):1775-8. doi: 10.1007/s11255-014-0708-z. Epub 2014 Apr 6. Int Urol Nephrol. 2014. PMID: 24705727
-
Surgical castration efficiently delays the time of starting a systemic chemotherapy in castration-resistant prostate cancer patients refractory to initial androgen-deprivation therapy.Prostate Int. 2015 Dec;3(4):123-6. doi: 10.1016/j.prnil.2015.10.015. Epub 2015 Oct 20. Prostate Int. 2015. PMID: 26779458 Free PMC article.
-
Beyond boundaries: unraveling innovative approaches to combat bone-metastatic cancers.Front Endocrinol (Lausanne). 2024 Jan 8;14:1260491. doi: 10.3389/fendo.2023.1260491. eCollection 2023. Front Endocrinol (Lausanne). 2024. PMID: 38260135 Free PMC article. Review.
-
Prostate Cancer for the Internist.N Am J Med Sci. 2015 Oct;7(10):429-35. doi: 10.4103/1947-2714.168660. N Am J Med Sci. 2015. PMID: 26713287 Free PMC article. Review.
References
-
- Huggins C, Hodges CV. Studies on prostatic cancer. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res. 1941;1:293–297. - PubMed
-
- Garcia JA, Rini BI. Castration-resistant prostate cancer: many treatments, many options, many challenges ahead. Cancer. 2012;118:2583–2593. - PubMed
-
- American Urological Association, authors. Prostate Cancer: Guideline for the Management of Clinically Localized Prostate Cancer: 2007 Update. [Accessed April 4, 2012]. http://www.auanet.org/content/clinical-practice-guidelines/clinical-guid....
-
- Heidenreich A, Bolla M, Joniau S, et al. Guidelines on Prostate Cancer. [Accessed April 4, 2012]. http://www.uroweb.org/gls/pdf/08_Prostate_CancerJuly6th.pdf.
-
- NCCN Clinical Practice Guides in Oncology: Prostate Cancer. [Accessed April 4, 2012]. http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf.
LinkOut - more resources
Full Text Sources