

Consenting options for posthumous organ donation: presumed consent and incentives are not favored
- PMID: 23173834
- PMCID: PMC3519501
- DOI: 10.1186/1472-6939-13-32
Consenting options for posthumous organ donation: presumed consent and incentives are not favored
Abstract
Background: Posthumous organ procurement is hindered by the consenting process. Several consenting systems have been proposed. There is limited information on public relative attitudes towards various consenting systems, especially in Middle Eastern/Islamic countries.
Methods: We surveyed 698 Saudi Adults attending outpatient clinics at a tertiary care hospital. Preference and perception of norm regarding consenting options for posthumous organ donation were explored. Participants ranked (1, most agreeable) the following, randomly-presented, options from 1 to 11: no-organ-donation, presumed consent, informed consent by donor-only, informed consent by donor-or-surrogate, and mandatory choice; the last three options ± medical or financial incentive.
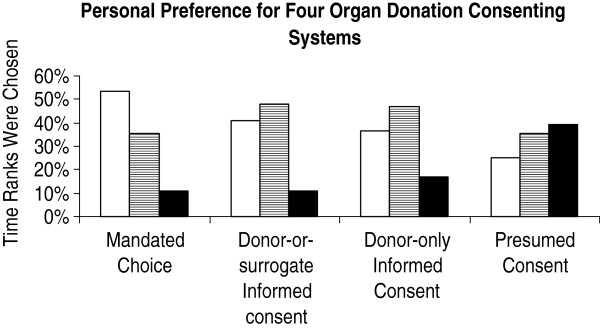
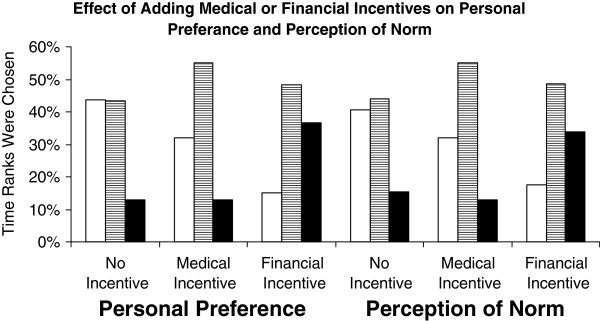
Results: Mean(SD) age was 32(9) year, 27% were males, 50% were patients' companions, 60% had ≥ college education, and 20% and 32%, respectively, knew an organ donor or recipient. Mandated choice was among the top three choices for preference of 54% of respondents, with an overall median[25%,75%] ranking score of 3[2,6], and was preferred over donor-or-surrogate informed consent (4[2,7], p < 0.001), donor-only informed consent (5[3,7], p < 0.001), and presumed consent (7[3,10], p < 0.001). The addition of a financial or medical incentive, respectively, reduced ranking of mandated choice to 7[4,9], p < 0.001, and 5[3,8], p < 0.001; for donor-or-surrogate informed consent to 7[5,9], p < 0.001, and 5[3,7], p = 0.004; and for donor-only informed consent to 8[6,10], p < 0.001, and 5[3,7], p = 0.56. Distribution of ranking score of perception of norm and preference were similar except for no-organ donation (11[7,11] vs. 11[6,11], respectively, p = 0.002). Compared to females, males more perceived donor-or-surrogate informed consent as the norm (3[1,6] vs. 5[3,7], p < 0.001), more preferred mandated choice with financial incentive option (6[3,8] vs. 8[4,9], p < 0.001), and less preferred mandated choice with medical incentive option (7[4,9] vs. 5[2,7], p < 0.001). There was no association between consenting options ranking scores and age, health status, education level, or knowing an organ donor or recipient.
Conclusions: We conclude that: 1) most respondents were in favor of posthumous organ donation, 2) mandated choice system was the most preferred and presumed consent system was the least preferred, 3) there was no difference between preference and perception of norm in consenting systems ranking, and 4) financial (especially in females) and medical (especially in males) incentives reduced preference.
Figures
Similar articles
-
Patients' perceived purpose of clinical informed consent: Mill's individual autonomy model is preferred.BMC Med Ethics. 2014 Jan 10;15:2. doi: 10.1186/1472-6939-15-2. BMC Med Ethics. 2014. PMID: 24406020 Free PMC article.
-
Information disclosure in clinical informed consent: "reasonable" patient's perception of norm in high-context communication culture.BMC Med Ethics. 2014 Jan 10;15:3. doi: 10.1186/1472-6939-15-3. BMC Med Ethics. 2014. PMID: 24406055 Free PMC article.
-
Saudi views on consenting for research on medical records and leftover tissue samples.BMC Med Ethics. 2010 Oct 18;11:18. doi: 10.1186/1472-6939-11-18. BMC Med Ethics. 2010. PMID: 20955580 Free PMC article.
-
[An ethical evaluation of presumed consent for organ donation in Switzerland].Rev Med Suisse. 2020 Feb 19;16(682):370-373. Rev Med Suisse. 2020. PMID: 32073773 Review. French.
-
Winning hearts and minds: using psychology to promote voluntary organ donation.Health Care Anal. 2000;8(2):101-21. doi: 10.1023/A:1009402628830. Health Care Anal. 2000. PMID: 11183441 Review.
Cited by
-
Egyptians' social acceptance and consenting options for posthumous organ donation; a cross sectional study.BMC Med Ethics. 2020 Jun 15;21(1):49. doi: 10.1186/s12910-020-00490-6. BMC Med Ethics. 2020. PMID: 32539704 Free PMC article.
-
Current state of ethical challenges reported in Saudi Arabia: a systematic review & bibliometric analysis from 2010 to 2021.BMC Med Ethics. 2022 Aug 13;23(1):82. doi: 10.1186/s12910-022-00816-6. BMC Med Ethics. 2022. PMID: 35964019 Free PMC article.
-
Factors underlying surrogate medical decision-making in middle eastern and east Asian women: a Q-methodology study.BMC Palliat Care. 2020 Sep 1;19(1):137. doi: 10.1186/s12904-020-00643-9. BMC Palliat Care. 2020. PMID: 32873284 Free PMC article.
-
Patients' perceived purpose of clinical informed consent: Mill's individual autonomy model is preferred.BMC Med Ethics. 2014 Jan 10;15:2. doi: 10.1186/1472-6939-15-2. BMC Med Ethics. 2014. PMID: 24406020 Free PMC article.
-
Information disclosure in clinical informed consent: "reasonable" patient's perception of norm in high-context communication culture.BMC Med Ethics. 2014 Jan 10;15:3. doi: 10.1186/1472-6939-15-3. BMC Med Ethics. 2014. PMID: 24406055 Free PMC article.
References
-
- Clark PAC. Financial Incentives for Cadaveric Organ Donation: An Ethical Analysis. The Internet Journal of Law, Healthcare and Ethics; 2006. p. 4(1).
-
- Kingdom of Saudi Arabia. Ministry of Health. Center for Organ Transplantation. Annual Report 2008. Available at Saudi Center for Organ Transplantation. [ http://www.scot.org.sa/en/], accessed 10 June 2012.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
