

Interlaboratory and interstudy reproducibility of a novel lateral-flow device and influence of antifungal therapy on detection of invasive pulmonary aspergillosis
- PMID: 23175252
- PMCID: PMC3553898
- DOI: 10.1128/JCM.02142-12
Interlaboratory and interstudy reproducibility of a novel lateral-flow device and influence of antifungal therapy on detection of invasive pulmonary aspergillosis
Abstract
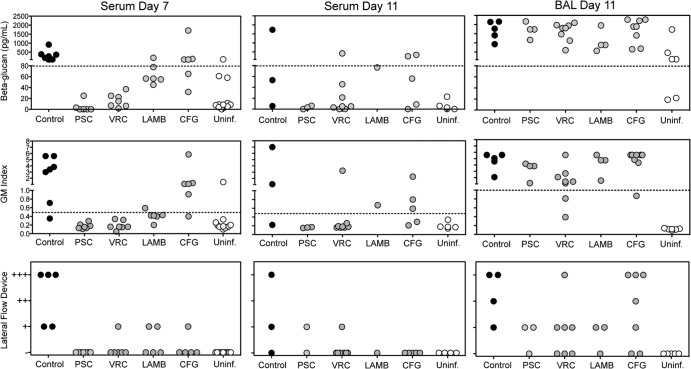
Interest in lateral-flow devices (LFDs) as potential point-of-care assays for the diagnosis of infectious diseases has increased. Our objective was to evaluate the interlaboratory and interstudy reproducibility and the effects of antifungal therapy on an LFD developed for invasive pulmonary aspergillosis (IPA) detection. An established neutropenic guinea pig model of IPA caused by Aspergillus fumigatus was used. At predetermined time points (1 h and 3, 5, and 7 days postinoculation), blood and bronchoalveolar lavage (BAL) fluid were collected from infected and uninfected animals. In a separate experiment, guinea pigs were treated with posaconazole (10 mg/kg of body weight orally [p.o.] twice a day [BID]), voriconazole (10 mg/kg p.o. BID), liposomal amphotericin B (10 mg/kg intraperitoneally [i.p.] once a day [QD]), or caspofungin (2 mg/kg i.p. QD), and samples were collected on days 7 and 11. Each laboratory independently evaluated the IgG monoclonal antibody-based LFD. Galactomannan and (1 → 3)-β-D-glucan were also measured using commercially available kits. Good interlaboratory agreement was observed with the LFD, as the results for 97% (32/33) of the serum and 78.8% (26/33) of the BAL fluid samples from infected animals were in agreement. Good interstudy agreement was also observed. The serum sensitivity of each surrogate-marker assay was reduced in animals treated with antifungals. In contrast, these markers remained elevated within the BAL fluids of treated animals, which was consistent with the fungal burden and histopathology results. These results demonstrate that the LFD assay is reproducible between different laboratories and studies. However, the sensitivity of this assay and other markers of IPA may be reduced with serum in the presence of antifungal therapy.
Figures

Comment in
-
Interlaboratory and interstudy reproducibility of a novel lateral-flow device: a statistical issue.J Clin Microbiol. 2013 May;51(5):1652. doi: 10.1128/JCM.00111-13. J Clin Microbiol. 2013. PMID: 23592858 Free PMC article. No abstract available.
-
Reply to "Interlaboratory and interstudy reproducibility of a novel lateral-flow device: a statistical issue".J Clin Microbiol. 2013 May;51(5):1653. doi: 10.1128/JCM.00366-13. J Clin Microbiol. 2013. PMID: 23592859 Free PMC article. No abstract available.
References
-
- Lin SJ, Schranz J, Teutsch SM. 2001. Aspergillosis case-fatality rate: systematic review of the literature. Clin. Infect. Dis. 32:358–366 - PubMed
-
- Caillot D, Casasnovas O, Bernard A, Couaillier JF, Durand C, Cuisenier B, Solary E, Piard F, Petrella T, Bonnin A, Couillault G, Dumas M, Guy H. 1997. Improved management of invasive pulmonary aspergillosis in neutropenic patients using early thoracic computed tomographic scan and surgery. J. Clin. Oncol. 15:139–147 - PubMed
-
- Garey KW, Rege M, Pai MP, Mingo DE, Suda KJ, Turpin RS, Bearden DT. 2006. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin. Infect. Dis. 43:25–31 - PubMed
-
- Greene RE, Schlamm HT, Oestmann JW, Stark P, Durand C, Lortholary O, Wingard JR, Herbrecht R, Ribaud P, Patterson TF, Troke PF, Denning DW, Bennett JE, de Pauw BE, Rubin RH. 2007. Imaging findings in acute invasive pulmonary aspergillosis: clinical significance of the halo sign. Clin. Infect. Dis. 44:373–379 - PubMed
-
- Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Segal BH, Steinbach WJ, Stevens DA, van Burik JA, Wingard JR, Patterson TF. 2008. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin. Infect. Dis. 46:327–360 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
