

Review
doi: 10.1016/j.cger.2012.09.005.
Altered mental status in older patients in the emergency department
Affiliations
- PMID: 23177603
- PMCID: PMC3614410
- DOI: 10.1016/j.cger.2012.09.005
Item in Clipboard
Review
Altered mental status in older patients in the emergency department
Clin Geriatr Med.
2013 Feb.
Abstract
Altered mental status is a common chief compliant among older patients in the emergency department (ED). Acute changes in mental status are more concerning and are usually secondary to delirium, stupor, and coma. Although stupor and coma are easily identifiable, the clinical presentation of delirium can be subtle and is often missed without actively screening for it. For patients with acute changes in mental status the ED evaluation should focus on searching for the underlying etiology. Infection is one of the most common precipitants of delirium, but multiple causes may exist concurrently.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
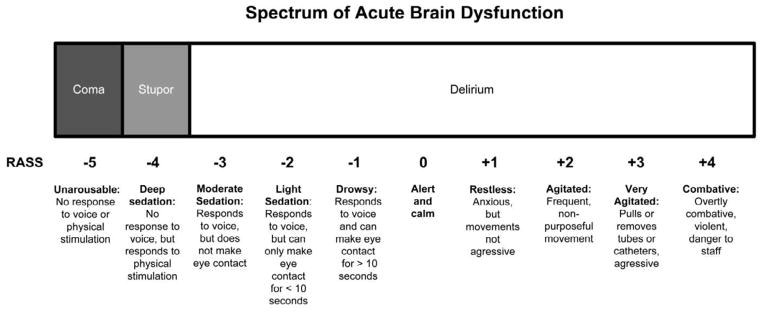
Spectrum of acute brain dysfunction based upon the Richmond Agitation Sedation Scale (RASS). Courtesy of Vanderbilt University, Nashville, TN. Copyright © 2012. Used with Permission.
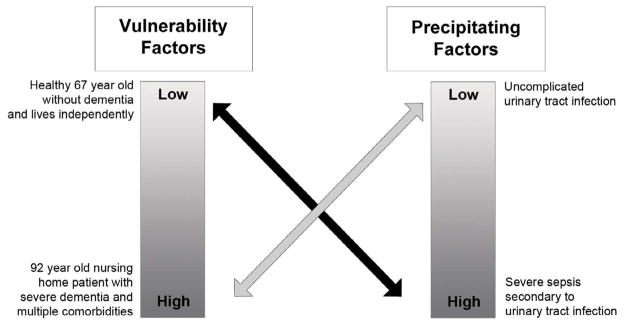
Interrelationship between patient vulnerability and precipitating factors for developing acute brain dysfunction such as delirium. Patients who not vulnerable require significant noxious stimuli to develop acute brain dysfunction (black arrow). Patients who are highly vulnerable require only minor noxious stimuli to develop acute brain dysfunction (gray arrow). Adapted from Inouye et al. JAMA 1996;275:852–857.
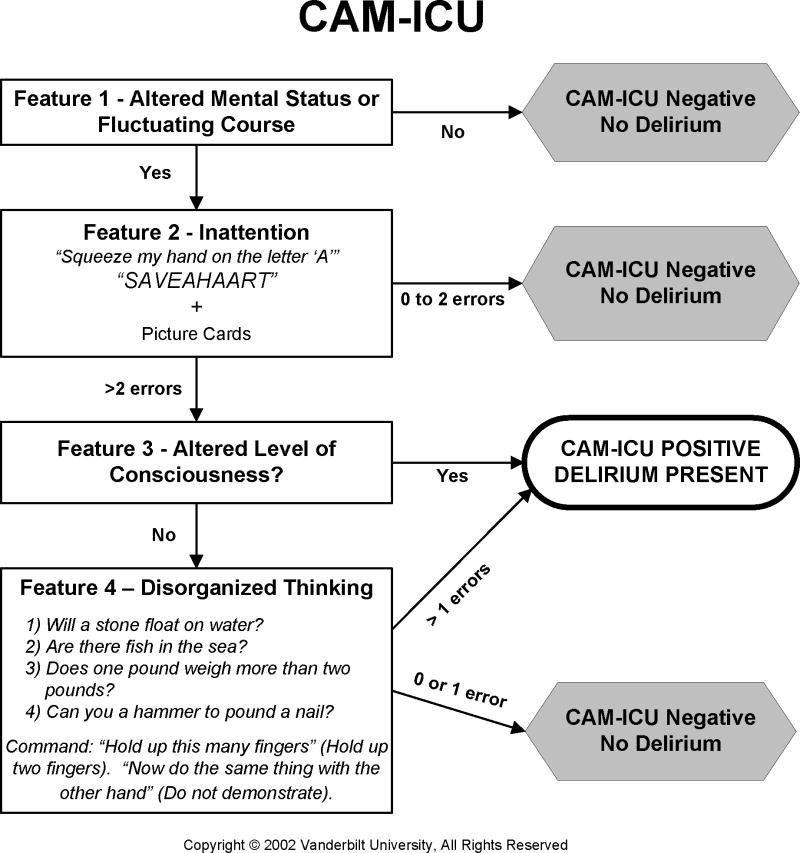
Confusion Assessment Method for the Intensive Care Unit. Adapted from www.icudelirium.org . Courtesy of Dr. Wes Ely and Vanderbilt University, Nashville, TN. Copyright © 2002. Used with Permission.
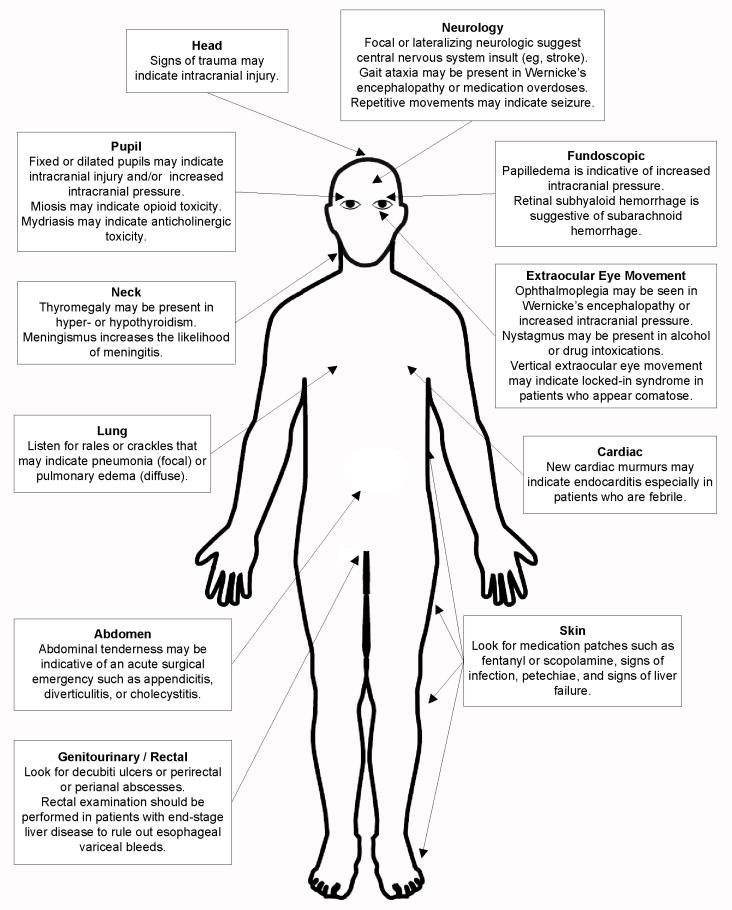
The physical examination of the patient with delirium, stupor, or coma.
References
-
- Morandi A, Pandharipande P, Trabucchi M, et al. Understanding international differences in terminology for delirium and other types of acute brain dysfunction in critically ill patients. Intensive Care Med. 2008;34(10):1907–1915. - PubMed
-
- Clarfield AM. The decreasing prevalence of reversible dementias: an updated meta-analysis. Arch Intern Med. 2003;163(18):2219–2229. - PubMed
-
- Schuur JD, Venkatesh AK. The growing role of emergency departments in hospital admissions. N Engl J Med. 2012;367(5):391–393. - PubMed
-
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl Health Stat Report. 2010;(26):1–31. - PubMed
-
- He W, Sengupta M, Velkoff VA, DeBarros KA. US Census Bureau, Current Population Reports, P23–209, 65+ in the United States: 2005. U.S. Government Printing Office; 2005.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
