

Early-onset Alzheimer's disease: nonamnestic subtypes and type 2 AD
- PMID: 23178565
- PMCID: PMC3532551
- DOI: 10.1016/j.arcmed.2012.11.009
Early-onset Alzheimer's disease: nonamnestic subtypes and type 2 AD
Abstract
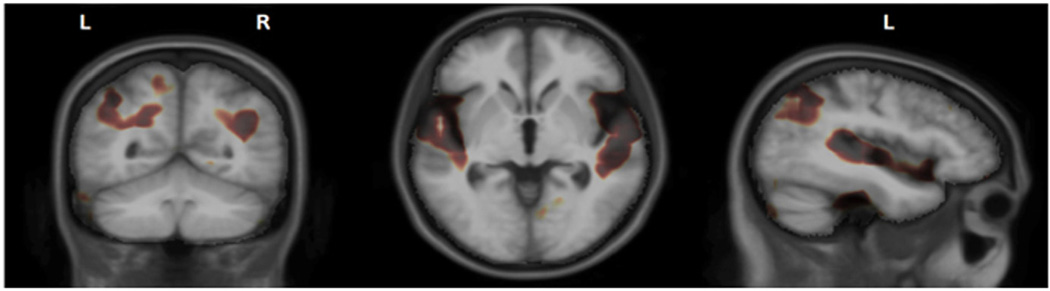
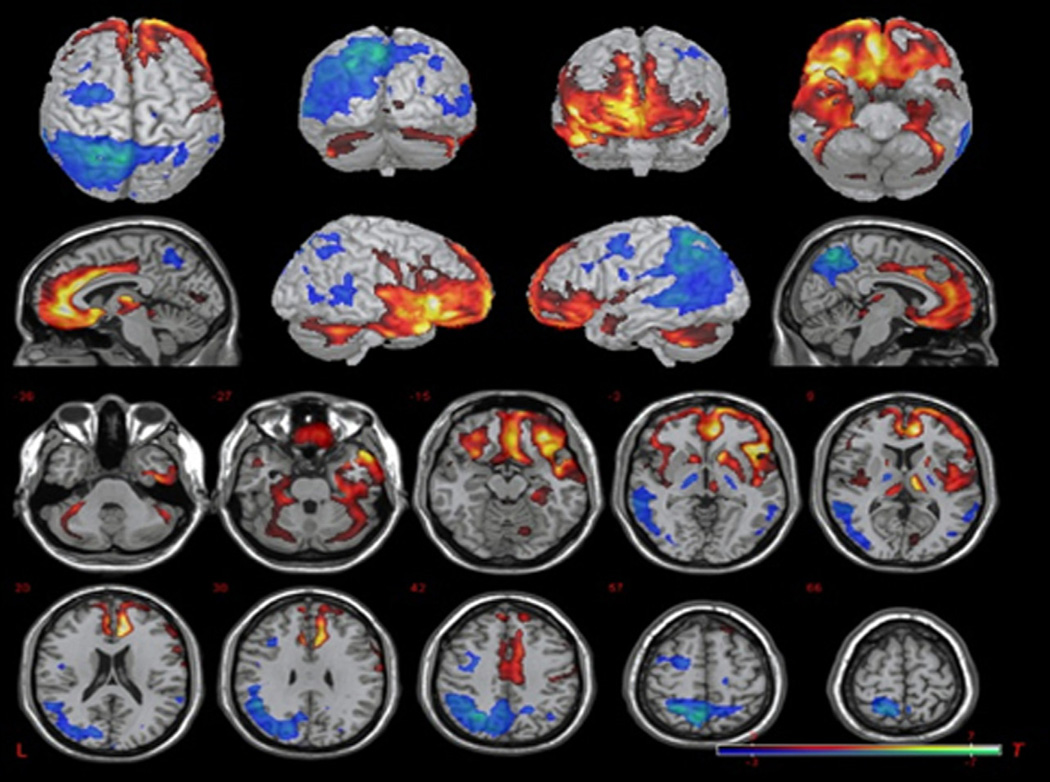
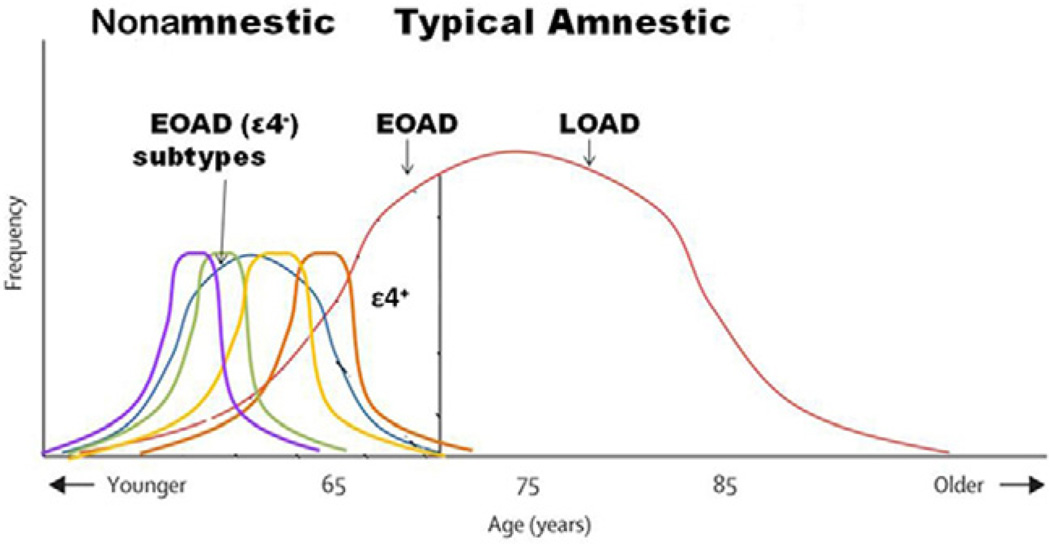
Patients with Alzheimer's disease (AD), the most prevalent neurodegenerative dementia, are usually elderly; however, ∼4-5% develop early-onset AD (EOAD) with onset before age 65. Most EOAD is sporadic, but about 5% of patients with EOAD have an autosomal dominant mutation such as Presenilin 1, Presenilin 2, or alterations in the Amyloid Precursor Protein gene. Although most Alzheimer's research has concentrated on older, late-onset AD (LOAD), there is much recent interest and research in EOAD. These recent studies indicate that EOAD is a heterogeneous disorder with significant differences from LOAD. From 22-64% of EOAD patients have a predominant nonamnestic syndrome presenting with deficits in language, visuospatial abilities, praxis, or other non-memory cognition. These nonamnestic patients may differ in several ways from the usual memory or amnestic patients. Patients with nonamnestic EOAD compared to typical amnestic AD have a more aggressive course, lack the apolipoprotein Eɛ4 (APOE ɛ4) susceptibility gene for AD, and have a focus and early involvement of non-hippocampal areas of brain, particularly parietal neocortex. These differences in the EOAD subtypes indicate differences in the underlying amyloid cascade, the prevailing pathophysiological theory for the development of AD. Together the results of recent studies suggest that nonamnestic subtypes of EOAD constitute a Type 2 AD distinct from the usual, typical disorder. In sum, the study of EOAD can reveal much about the clinical heterogeneity, predisposing factors, and neurobiology of this disease.
Copyright © 2012 IMSS. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Alzheimer A, Stelzmann RA, Schnitzlein HN, et al. An English translation of Alzheimer’s 1907 paper, Uber eine eigenartige Erkankung der Hirnrinde. Clin Anat. 1995;8:429–431. - PubMed
-
- Blessed G, Tomlinson BE, Roth M. The association between quantitative measures of dementia and of senile change in the cerebral grey matter of elderly subjects. Br J Psychiatry. 1968;114:797–811. - PubMed
-
- Katzman R. Editorial: The prevalence and malignancy of Alzheimer disease. A major killer. Arch Neurol. 1976;33:217–218. - PubMed
-
- McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34:939–944. - PubMed
-
- Querfurth HW, LaFerla FM. Alzheimer’s disease. N Engl J Med. 2010;362:329–344. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
