

Trans-Oral Video-Assisted Neck Surgery (TOVANS). A new transoral technique of endoscopic thyroidectomy with gasless premandible approach
- PMID: 23179070
- PMCID: PMC3599170
- DOI: 10.1007/s00464-012-2588-6
Trans-Oral Video-Assisted Neck Surgery (TOVANS). A new transoral technique of endoscopic thyroidectomy with gasless premandible approach
Abstract
Background: Endoscopic thyroidectomy is a well-established surgical technique. We have been utilizing precordial video-assisted neck surgery (VANS) with a gasless anterior neck skin lifting method. Recently, natural orifice transluminal endoscopic surgery (NOTES) has generated excitement among surgeons as potentially scar-free surgery. We developed an innovative gasless transoral technique for endoscopic thyroidectomy that incorporated the concept of NOTES in a VANS-technique.
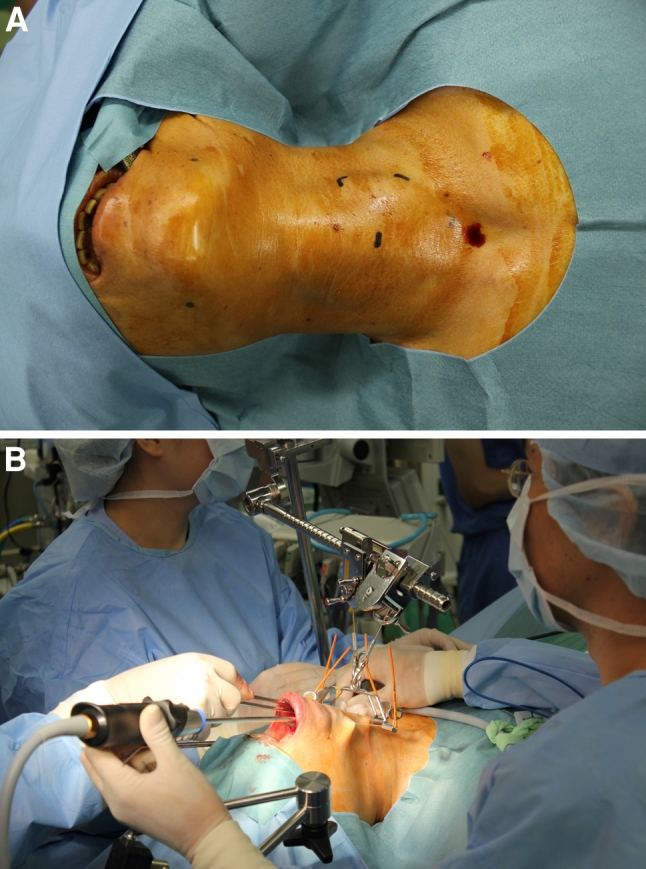
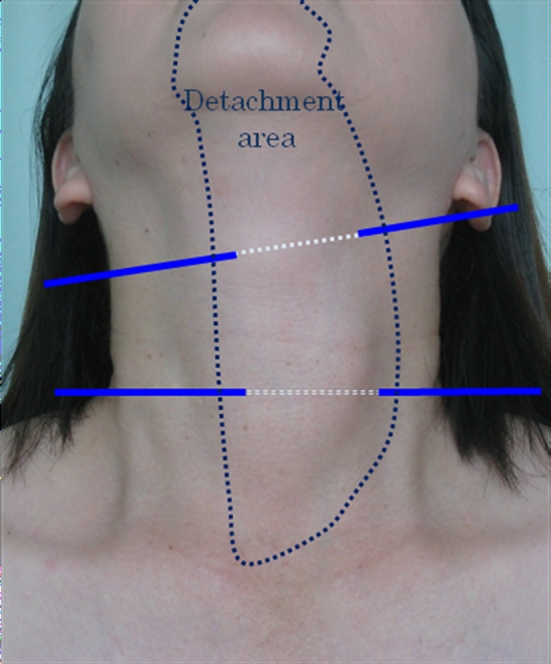
Methods: Incision was made at the vestibulum under the inferior lip. From the vestibulum to the anterior cervical region, a subplatysmal tunnel in front of the mandible was created and cervical skin was lifted by Kirschner wires and a mechanical retracting system. This method without CO2 insufflation created an effective working space and provided an excellent cranio-caudal view so that we could perform thyroidectomy and central node dissection safely.
Results: Beginning with our first clinical application of TOVANS in September 2009, we have performed eight such procedures. Three of the eight patients had papillary microcarcinoma and received central node dissection after thyroidectomy. All patients began oral intake 1 day after surgery. The sensory disorder around the chin persisted more than 6 months after surgery in all patients. Recurrent laryngeal nerve palsy revealed in one patient. Nobody had mental nerve palsy, and no infection developed with use of preventive antibacterial tablets for 3 days.
Conclusions: We developed a new method for gasless transoral endoscopic thyroidectomy with a premandible approach and anterior neck-skin lifting. TOVANS makes possible complete endoscopic radical lymphadenectomy for papillary thyroid cancer. We believe that this method is innovative and progressive and has not only a cosmetic advantage but also provides easy access to the central node compartment for dissection in endoscopic thyroid cancer surgery.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
