

Should home-based HIV testing and counseling services be offered periodically in programs of ARV treatment as prevention? A case study in Likoma (Malawi)
- PMID: 23180155
- PMCID: PMC3619025
- DOI: 10.1007/s10461-012-0365-0
Should home-based HIV testing and counseling services be offered periodically in programs of ARV treatment as prevention? A case study in Likoma (Malawi)
Abstract
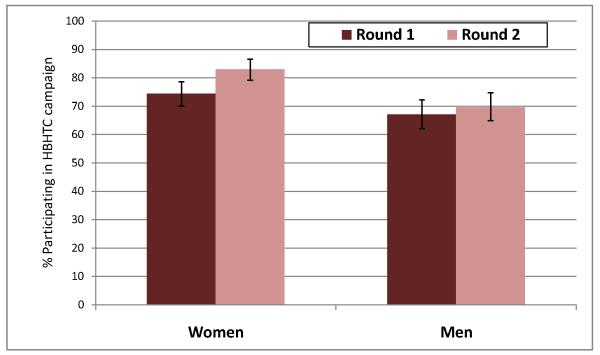
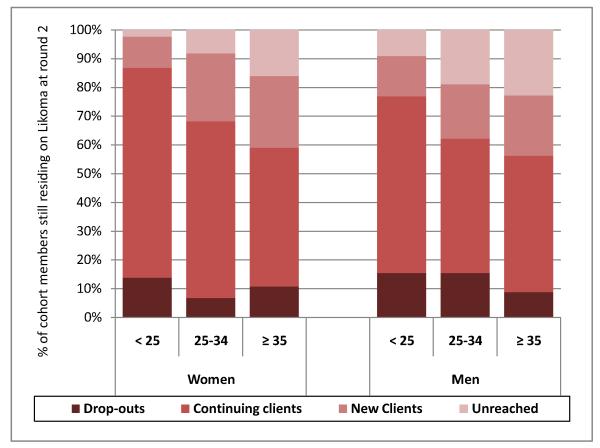
To reduce HIV incidence, prevention programs centered on the use of antiretrovirals require scaling-up HIV testing and counseling (HTC). Home-based HTC services (HBHTC) increase HTC coverage, but HBHTC has only been evaluated during one-off campaigns. Two years after an initial HBHTC campaign ("round 1"), we conducted another HBHTC campaign ("round 2") in Likoma (Malawi). HBHTC participation increased during round 2 among women (from 74 to 83%, P < 0.01). New HBHTC clients were recruited, especially at ages 25 and older. Only 6.9% of women but 15.9% of men remained unreached by HBHTC after round 2. HIV prevalence during round 2 was low among clients who were HIV-negative during round 1 (0.7%), but high among women who received their first ever HIV test during round 2 (42.8%). The costs per newly diagnosed infection increased significantly during round 2. Periodically conducting HBHTC campaigns can further increase HTC, but supplementary interventions to enroll individuals not reached by HBHTC are needed.
Figures
References
-
- Roth DL, Stewart KE, Clay OJ, van Der Straten A, Karita E, Allen S. Sexual practices of HIV discordant and concordant couples in Rwanda: effects of a testing and counselling programme for men. Int J STD AIDS. 2001 Mar;12(3):181–8. - PubMed
-
- Allen S, Meinzen-Derr J, Kautzman M, Zulu I, Trask S, Fideli U, et al. Sexual behavior of HIV discordant couples after HIV counseling and testing. AIDS. 2003 Mar 28;17(5):733–40. - PubMed
-
- Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009 Jan 3;373(9657):48–57. - PubMed
-
- WHO . Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector. World Health Organization; Geneva: 2010.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
