

Portal biliopathy
- PMID: 23180936
- PMCID: PMC3501764
- DOI: 10.3748/wjg.v18.i43.6177
Portal biliopathy
Abstract
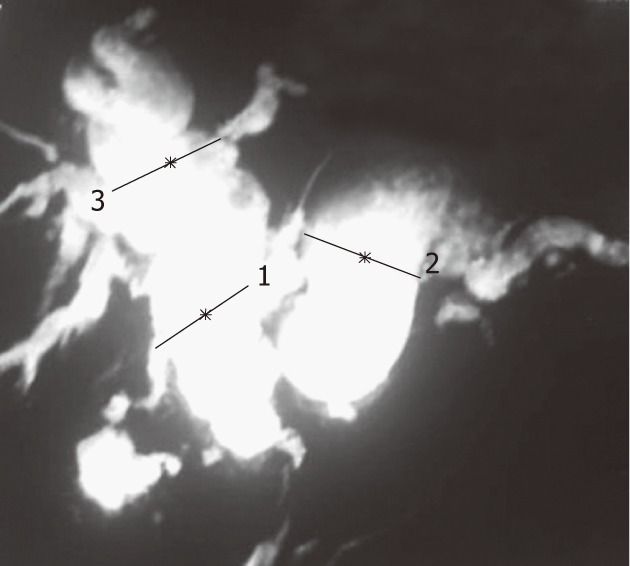
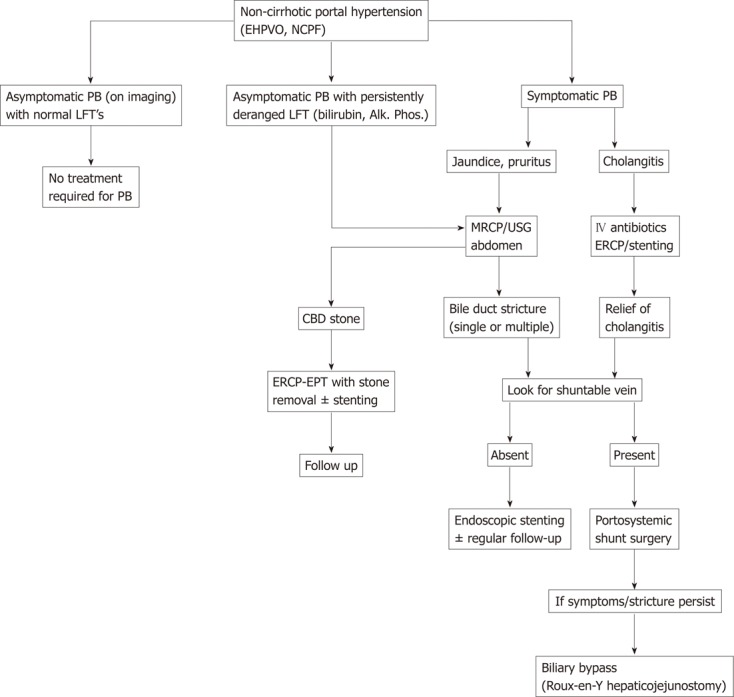
Biliary ductal changes are a common radiological finding in patients with portal hypertension, however only a small percentage of patients (5%-30%) develop symptomatic bile duct obstruction. The exact pathogenesis is not clear, but an involvement of factors such as bile duct compression by venous collaterals, ischemia, and infection is accepted by most authors. Although endoscopic retrograde cholangiopancreatography was used to define and diagnose this condition, magnetic resonance cholangiopancreatography is currently the investigation of choice for diagnosing this condition. Treatment is indicated only for symptomatic cases. Portosystemic shunts are the treatment of choice for symptomatic portal biliopathy. In the majority of patients, the changes caused by biliopathy resolve after shunt surgery, however, 15%-20% patients require a subsequent bilio-enteric bypass or endoscopic management for persistent biliopathy. There is a role for endoscopic therapy in patients with bile duct stones, cholangitis or when portosystemic shunt surgery is not feasible.
Keywords: Biliary obstruction; Extrahepatic portal venous obstruction; Non cirrhotic portal fibrosis; Portal cavernoma; Proximal lienorenal shunt; Pseudosclerosing cholangitis.
Figures
References
-
- Chandra R, Kapoor D, Tharakan A, Chaudhary A, Sarin SK. Portal biliopathy. J Gastroenterol Hepatol. 2001;16:1086–1092. - PubMed
-
- Fraser J, Brown AK. A clinical syndrome associated with a rare anomaly of the vena portae system. Surg Gynecol Obstet. 1944;78:520–524.
-
- Gibson JB, Richards RL. Cavernous transformation of the portal vein. J Pathol Bacteriol. 1955;70:81–96. - PubMed
-
- Hunt AH. Compression of the common bile-duct by an enlarging collateral vein in a case of portal hypertension. Br J Surg. 1965;52:636–637. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
