

Determinants of kidney oxygen consumption and their relationship to tissue oxygen tension in diabetes and hypertension
- PMID: 23181475
- PMCID: PMC3951849
- DOI: 10.1111/1440-1681.12034
Determinants of kidney oxygen consumption and their relationship to tissue oxygen tension in diabetes and hypertension
Abstract
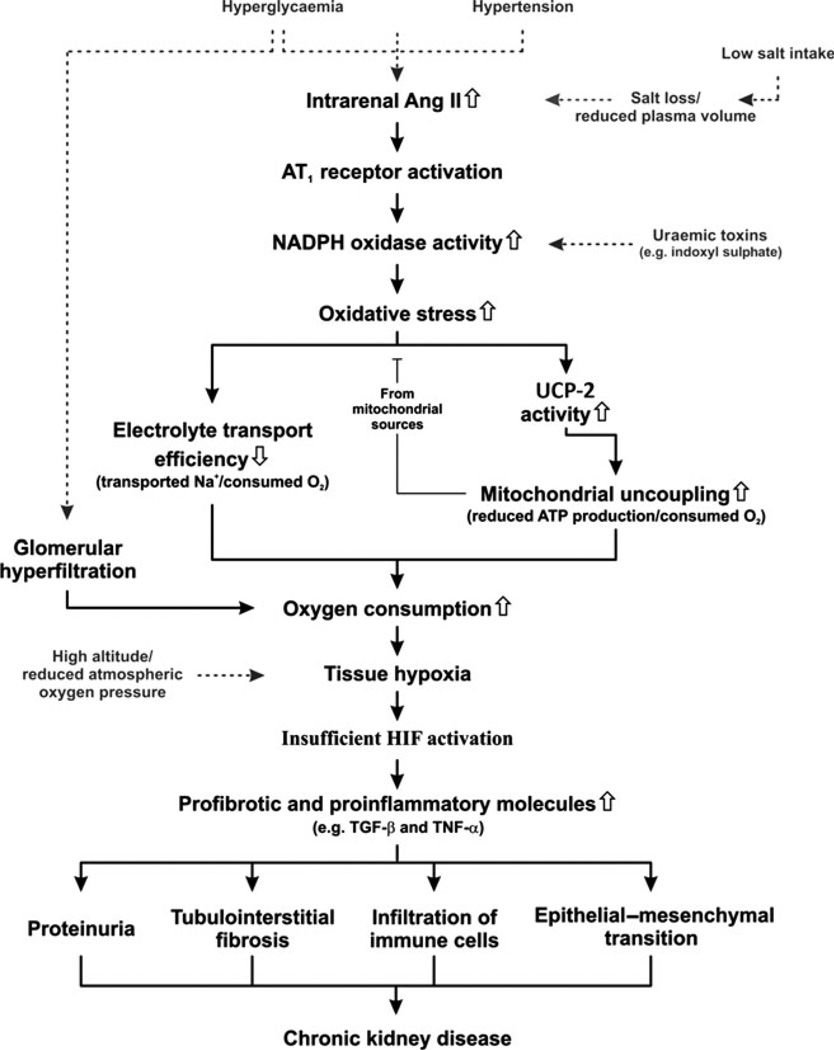
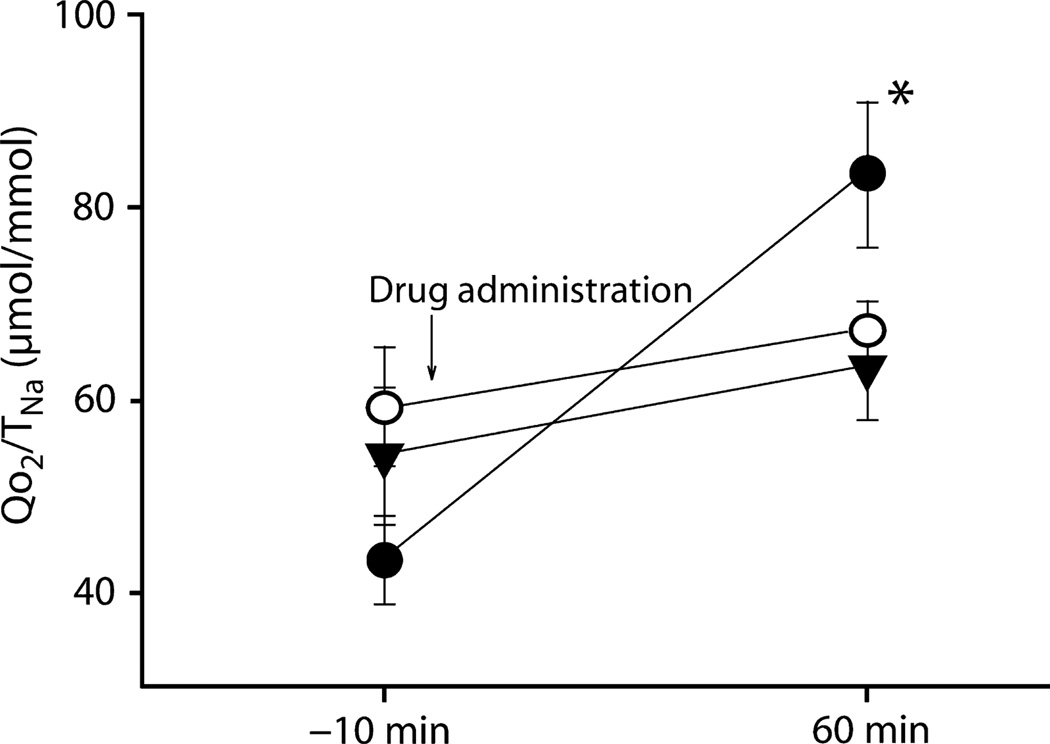
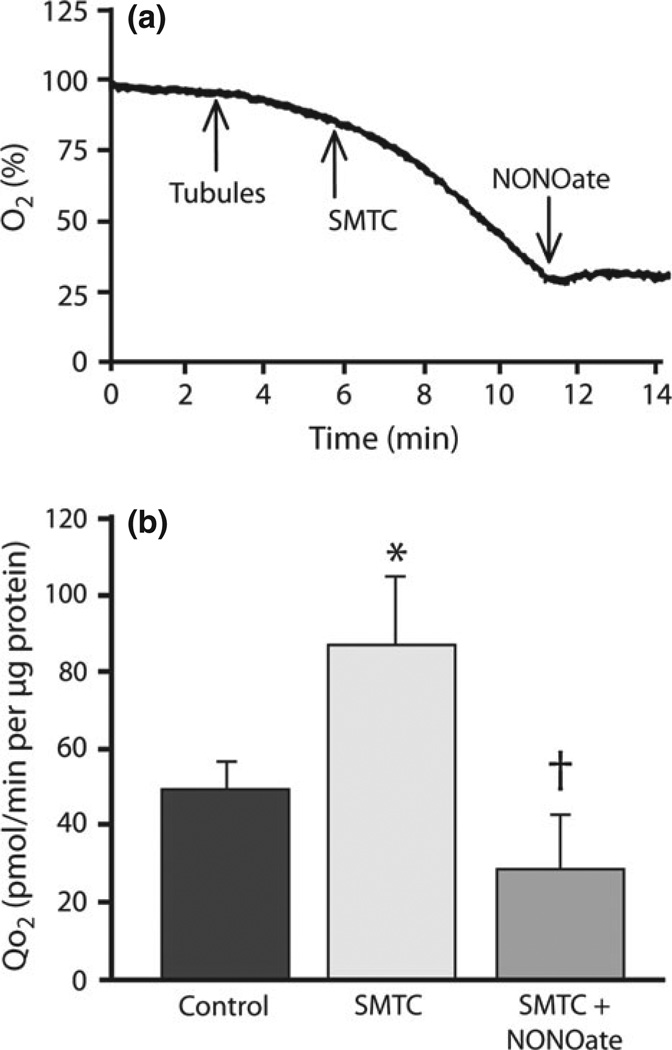
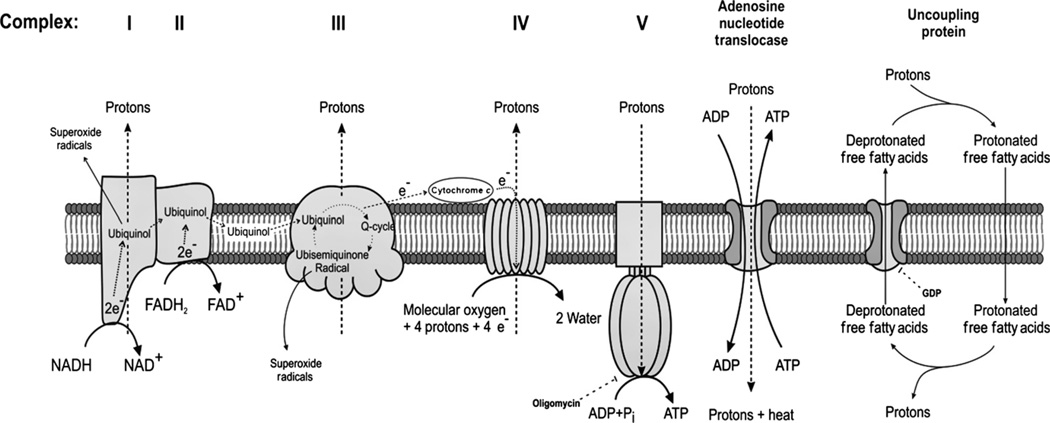
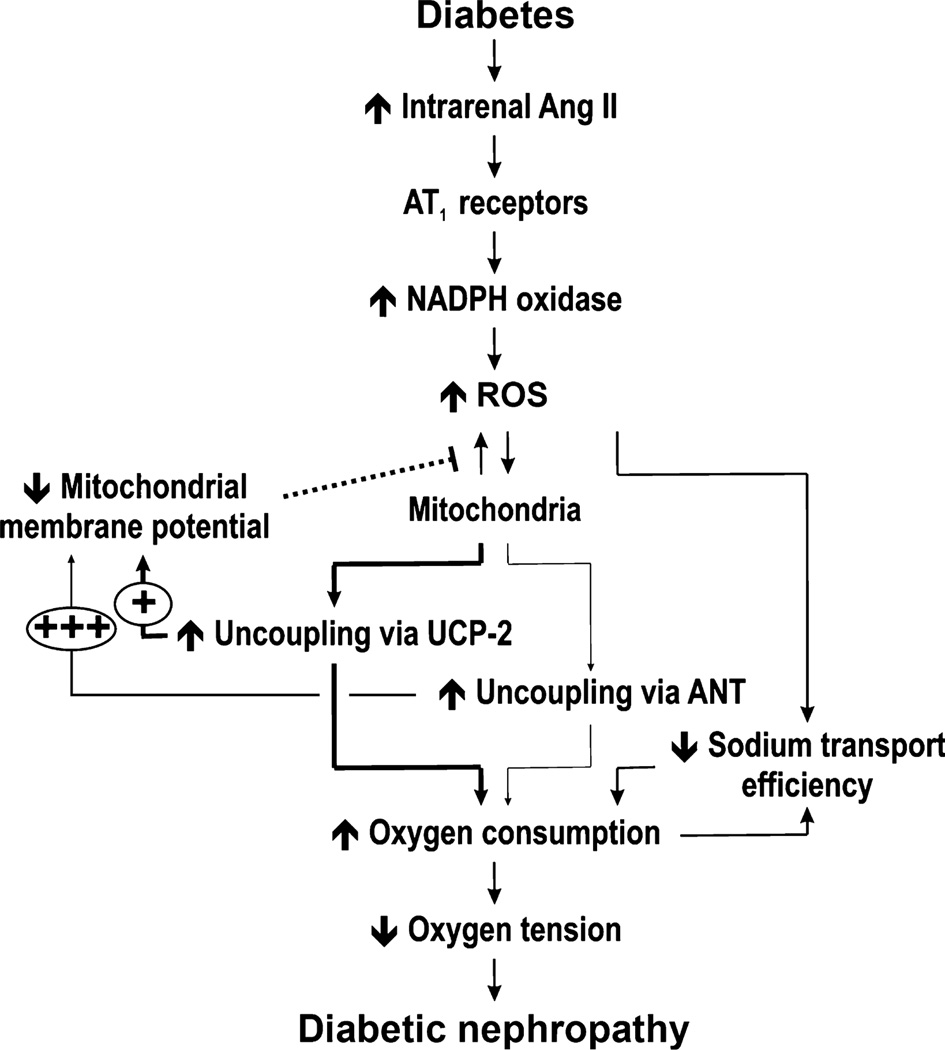
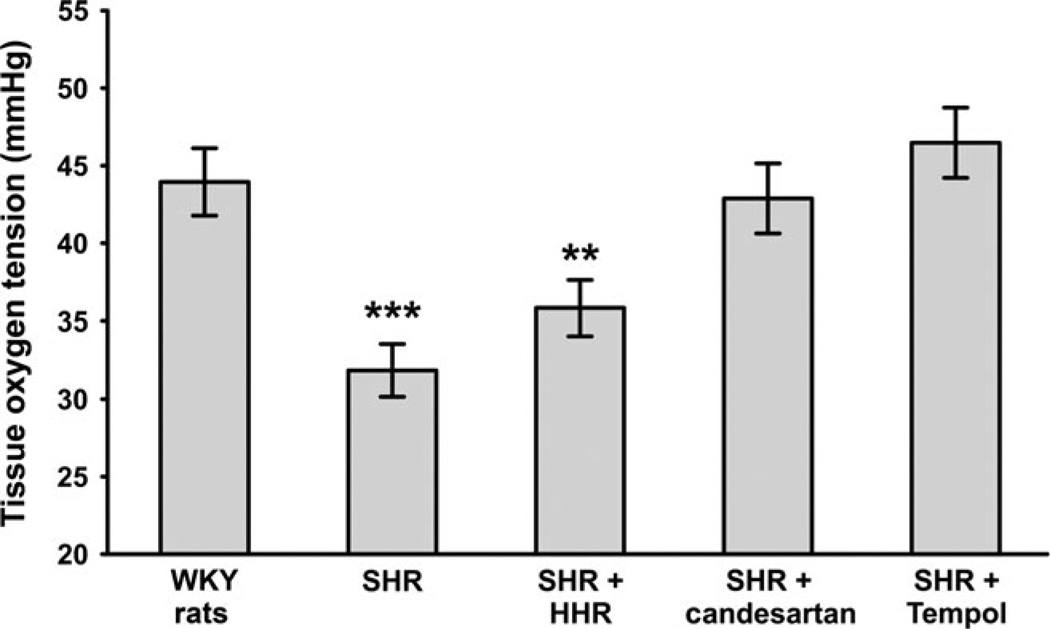
The high renal oxygen (O(2) ) demand is associated primarily with tubular O(2) consumption (Qo(2) ) necessary for solute reabsorption. Increasing O(2) delivery relative to demand via increased blood flow results in augmented tubular electrolyte load following elevated glomerular filtration, which, in turn, increases metabolic demand. Consequently, elevated kidney metabolism results in decreased tissue oxygen tension. The metabolic efficiency for solute transport (Qo(2) /T(Na) ) varies not only between different nephron sites, but also under different conditions of fluid homeostasis and disease. Contributing mechanisms include the presence of different Na(+) transporters, different levels of oxidative stress and segmental tubular dysfunction. Sustained hyperglycaemia results in increased kidney Qo(2) , partly due to mitochondrial dysfunction and reduced electrolyte transport efficiency. This results in intrarenal tissue hypoxia because the increased Qo(2) is not matched by a similar increase in O(2) delivery. Hypertension leads to renal hypoxia, mediated by increased angiotensin receptor tonus and oxidative stress. Reduced uptake in the proximal tubule increases load to the thick ascending limb. There, the increased load is reabsorbed, but at greater O(2) cost. The combination of hypertension, angiotensin II and oxidative stress initiates events leading to renal damage and reduced function. Tissue hypoxia is now recognized as a unifying pathway to chronic kidney disease. We have gained good knowledge about major changes in O(2) metabolism occurring in diabetic and hypertensive kidneys. However, further efforts are needed to elucidate how these alterations can be prevented or reversed before translation into clinical practice.
© 2012 The Authors Clinical and Experimental Pharmacology and Physiology © 2012 Wiley Publishing Asia Pty Ltd.
Figures
References
-
- Levy MN. Effect of variations of blood flow on renal oxygen extraction. Am. J. Physiol. 1960;199:13–18. - PubMed
-
- Eckardt KU, Bernhardt WM, Weidemann A, et al. Role of hypoxia in the pathogenesis of renal disease. Kidney Int. Suppl. 2005;99:S46–S51. - PubMed
-
- Eckardt KU, Rosenberger C, Jurgensen JS, Wiesener MS. Role of hypoxia in the pathogenesis of renal disease. Blood Purif. 2003;21:253–257. - PubMed
-
- Leong CL, Anderson WP, O’Connor PM, Evans RG. Evidence that renal arterial–venous oxygen shunting contributes to dynamic regulation of renal oxygenation. Am. J. Physiol. Renal Physiol. 2007;292:F1726–F1733. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
