

RTOG 0211: a phase 1/2 study of radiation therapy with concurrent gefitinib for newly diagnosed glioblastoma patients
- PMID: 23182702
- PMCID: PMC4199329
- DOI: 10.1016/j.ijrobp.2012.10.008
RTOG 0211: a phase 1/2 study of radiation therapy with concurrent gefitinib for newly diagnosed glioblastoma patients
Abstract
Purpose: To determine the safety and efficacy of gefitinib, an epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor, in combination with radiation for newly diagnosed glioblastoma (GBM) patients.
Methods and materials: Between March 21, 2002, and May 3, 2004, Radiation Therapy Oncology Group (RTOG) 0211 enrolled 31 and 147 GBM patients in the phase 1 and 2 arms, respectively. Treatment consisted of daily oral gefinitnib started at the time of conventional cranial radiation therapy (RT) and continued post RT for 18 months or until progression. Tissue microarrays from 68 cases were analyzed for EGFR expression.
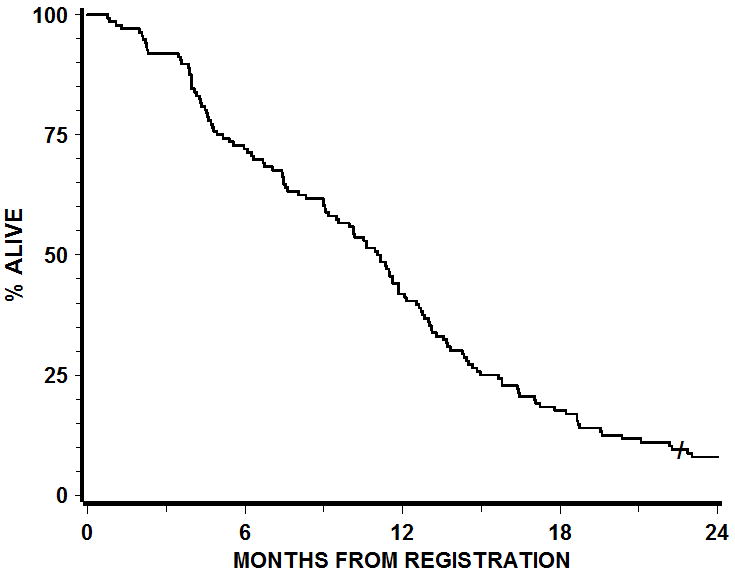
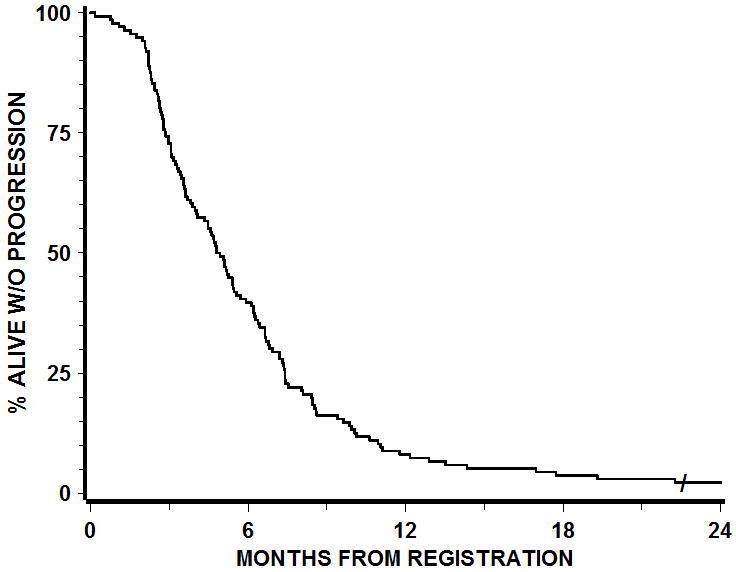
Results: The maximum tolerated dose (MTD) of gefitinib was determined to be 500 mg in patients on non-enzyme-inducing anticonvulsant drugs (non-EIAEDs). All patients in the phase 2 component were treated at a gefitinib dose of 500 mg; patients receiving EIADSs could be escalated to 750 mg. The most common side effects of gefitinib in combination with radiation were dermatologic and gastrointestinal. Median survival was 11.5 months for patients treated per protocol. There was no overall survival benefit for patients treated with gefitinib + RT when compared with a historical cohort of patients treated with RT alone, matched by RTOG recursive partitioning analysis (RPA) class distribution. Younger age was significantly associated with better outcome. Per protocol stratification, EGFR expression was not found to be of prognostic value for gefitinib + RT-treated patients.
Conclusions: The addition of gefitinib to RT is well tolerated. Median survival of RTOG 0211 patients treated with RT with concurrent and adjuvant gefitinib was similar to that in a historical control cohort treated with radiation alone.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
Comment in
-
In regard to Chakravarti et al.Int J Radiat Oncol Biol Phys. 2013 Jul 1;86(3):398-9. doi: 10.1016/j.ijrobp.2013.02.029. Int J Radiat Oncol Biol Phys. 2013. PMID: 23708078 No abstract available.
References
-
- Buckner JC, Ballman KV, Michalak JC, et al. Phase III trial of carmustine and cisplatin compared with carmustine alone and standard radiation therapy or accelerated radiation therapy in patients with glioblastoma multiforme: North Central Cancer Treatment Group 93-72-52 and Southwest Oncology Group 9503 Trials. J Clin Oncol. 2006;24(24):3871–9. - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–66. - PubMed
-
- Keime-Guibert F, Chinot O, Taillandier L, et al. Radiotherapy for glioblastoma in the elderly. N Engl J Med. 2007;356(15):1527–35. - PubMed
-
- Walker MD, Alexander E, Jr, Hunt WE, et al. Evaluation of BCNU and/or radiotherapy in the treatment of anaplastic gliomas. A cooperative clinical trial. J Neurosurg. 1978;49(3):333–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
