

Cost-effectiveness of alternating magnetic resonance imaging and digital mammography screening in BRCA1 and BRCA2 gene mutation carriers
- PMID: 23184400
- PMCID: PMC3586945
- DOI: 10.1002/cncr.27864
Cost-effectiveness of alternating magnetic resonance imaging and digital mammography screening in BRCA1 and BRCA2 gene mutation carriers
Abstract
Background: Current clinical guidelines recommend earlier, more intensive breast cancer screening with both magnetic resonance imaging (MRI) and mammography for women with breast cancer susceptibility gene (BRCA) mutations. Unspecified details of screening schedules are a challenge for implementing guidelines.
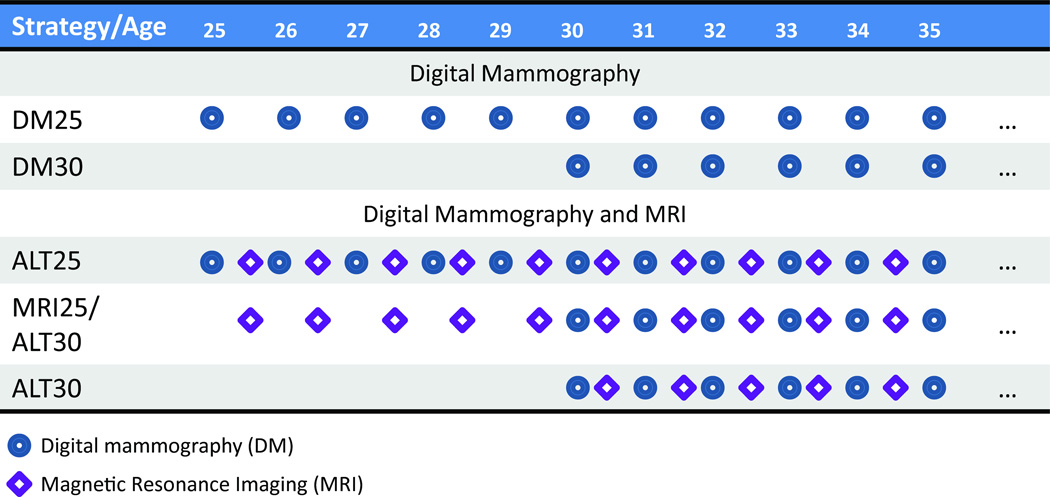
Methods: A Markov Monte Carlo computer model was used to simulate screening in asymptomatic women who were BRCA1 and BRCA2 mutation carriers. Three dual-modality strategies were compared with digital mammography (DM) alone: 1) DM and MRI alternating at 6-month intervals beginning at age 25 years (Alt25), 2) annual MRI beginning at age 25 years with alternating DM added at age 30 years (MRI25/Alt30), and 3) DM and MRI alternating at 6-month intervals beginning at age 30 years (Alt30). Primary outcomes were quality-adjusted life years (QALYs), lifetime costs (in 2010 US dollars), and incremental cost-effectiveness (dollars per QALY gained). Additional outcomes included potential harms of screening, and lifetime costs stratified into component categories (screening and diagnosis, treatment, mortality, and patient time costs).
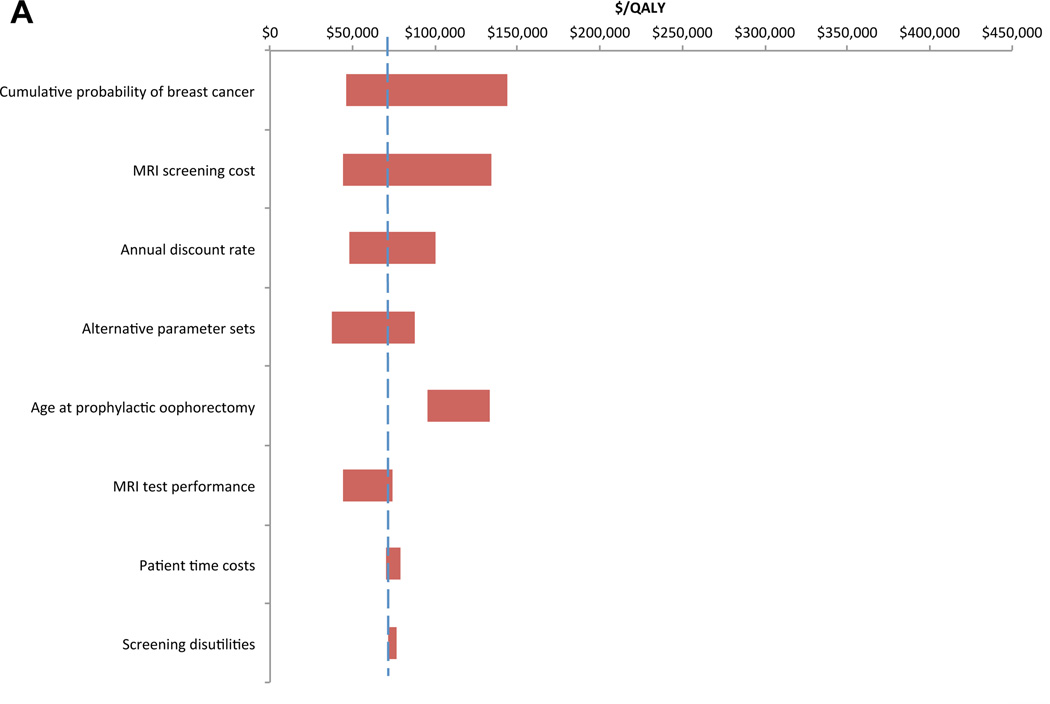
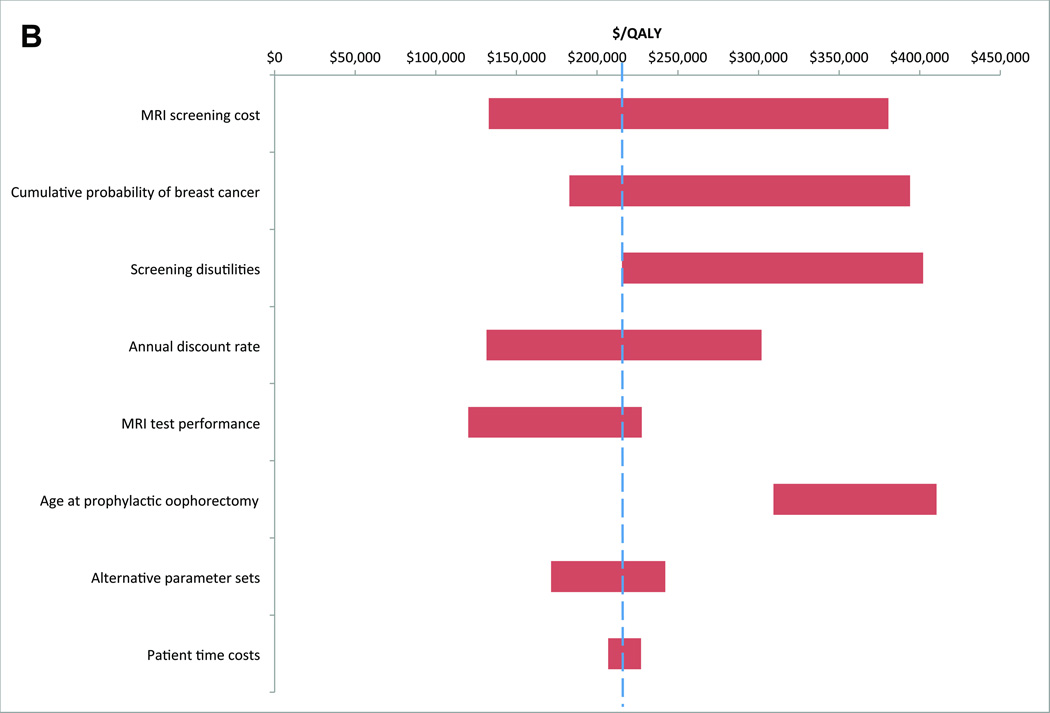
Results: All 3 dual-modality screening strategies increased QALYs and costs. Alt30 screening had the lowest incremental costs per additional QALY gained (BRCA1, $74,200 per QALY; BRCA2, $215,700 per QALY). False-positive test results increased substantially with dual-modality screening and occurred more frequently in BRCA2 carriers. Downstream savings in both breast cancer treatment and mortality costs were outweighed by increases in up-front screening and diagnosis costs. The results were influenced most by estimates of breast cancer risk and MRI costs.
Conclusions: Alternating MRI and DM screening at 6-month intervals beginning at age 30 years was identified as a clinically effective approach to applying current guidelines, and was more cost-effective in BRCA1 gene mutation carriers compared with BRCA2 gene mutation carriers.
Copyright © 2012 American Cancer Society.
Conflict of interest statement
Figures
Similar articles
-
Cost-effectiveness of screening BRCA1/2 mutation carriers with breast magnetic resonance imaging.JAMA. 2006 May 24;295(20):2374-84. doi: 10.1001/jama.295.20.2374. JAMA. 2006. PMID: 16720823
-
Annual screening strategies in BRCA1 and BRCA2 gene mutation carriers: a comparative effectiveness analysis.Cancer. 2012 Apr 15;118(8):2021-30. doi: 10.1002/cncr.26424. Epub 2011 Sep 20. Cancer. 2012. PMID: 21935911 Free PMC article.
-
Cost-effectiveness of MRI for breast cancer screening in BRCA1/2 mutation carriers.BMC Cancer. 2013 Jul 10;13:339. doi: 10.1186/1471-2407-13-339. BMC Cancer. 2013. PMID: 23837641 Free PMC article.
-
Dynamic contrast-enhanced magnetic resonance imaging for risk-stratified screening in women with BRCA mutations or high familial risk for breast cancer: are we there yet?Breast Cancer Res Treat. 2020 Sep;183(2):243-250. doi: 10.1007/s10549-020-05759-3. Epub 2020 Jul 3. Breast Cancer Res Treat. 2020. PMID: 32621252 Review.
-
Cost-effectiveness of mammography, MRI, and ultrasonography for breast cancer screening.Radiol Clin North Am. 2010 Sep;48(5):879-91. doi: 10.1016/j.rcl.2010.06.002. Radiol Clin North Am. 2010. PMID: 20868891 Review.
Cited by
-
"High-Risk Breast Cancer Screening in BRCA1/2 Carriers Leads to Early Detection and Improved Survival After a Breast Cancer Diagnosis".Front Oncol. 2021 Sep 2;11:683656. doi: 10.3389/fonc.2021.683656. eCollection 2021. Front Oncol. 2021. PMID: 34540661 Free PMC article.
-
Familial history and prevalence of BRCA1, BRCA2 and TP53 pathogenic variants in HBOC Brazilian patients from a public healthcare service.Sci Rep. 2022 Nov 3;12(1):18629. doi: 10.1038/s41598-022-23012-3. Sci Rep. 2022. PMID: 36329109 Free PMC article.
-
Optimal Screening in Breast Cancer Survivors With Dense Breasts on Mammography.J Clin Oncol. 2020 Nov 20;38(33):3833-3840. doi: 10.1200/JCO.20.01641. Epub 2020 Jul 24. J Clin Oncol. 2020. PMID: 32706641 Free PMC article.
-
Contralateral Prophylactic Mastectomy Consensus Statement from the American Society of Breast Surgeons: Additional Considerations and a Framework for Shared Decision Making.Ann Surg Oncol. 2016 Oct;23(10):3106-11. doi: 10.1245/s10434-016-5408-8. Epub 2016 Jul 28. Ann Surg Oncol. 2016. PMID: 27469118 Free PMC article. No abstract available.
-
Economic evaluation of breast MRI in screening - a systematic review and basic approach to cost-effectiveness analyses.Front Oncol. 2023 Dec 7;13:1292268. doi: 10.3389/fonc.2023.1292268. eCollection 2023. Front Oncol. 2023. PMID: 38130995 Free PMC article.
References
-
- NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Version 2.2011. 2011
-
- Lee CH, Dershaw DD, Kopans D, et al. Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer. J Am Coll Radiol. 2010;7:18–27. - PubMed
-
- Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75–89. - PubMed
-
- Warner E, Messersmith H, Causer P, et al. Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Ann Intern Med. 2008;148:671–679. - PubMed
Publication types
MeSH terms
Grants and funding
- U01CA69976/CA/NCI NIH HHS/United States
- U01 CA070040/CA/NCI NIH HHS/United States
- U01CA70013/CA/NCI NIH HHS/United States
- U01 CA086082/CA/NCI NIH HHS/United States
- U01CA63736/CA/NCI NIH HHS/United States
- U01CA86082/CA/NCI NIH HHS/United States
- R00 CA126147/CA/NCI NIH HHS/United States
- K07-CA128816/CA/NCI NIH HHS/United States
- K25 CA133141/CA/NCI NIH HHS/United States
- U01 CA063740/CA/NCI NIH HHS/United States
- U01CA70040/CA/NCI NIH HHS/United States
- U01CA63740/CA/NCI NIH HHS/United States
- U01 CA063731/CA/NCI NIH HHS/United States
- U01 CA086076/CA/NCI NIH HHS/United States
- U01 CA069976/CA/NCI NIH HHS/United States
- U01CA86076/CA/NCI NIH HHS/United States
- K25-CA133141/CA/NCI NIH HHS/United States
- U01 CA063736/CA/NCI NIH HHS/United States
- U01 CA070013/CA/NCI NIH HHS/United States
- K07 CA128816/CA/NCI NIH HHS/United States
- U01CA63731/CA/NCI NIH HHS/United States
- R00-CA126147/CA/NCI NIH HHS/United States
- HHSN261201100031C/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
