

Incidence and predictors of phantom shocks in implantable cardioverter defibrillator recipients
- PMID: 23184599
- PMCID: PMC3673601
- DOI: 10.1007/s12471-012-0345-z
Incidence and predictors of phantom shocks in implantable cardioverter defibrillator recipients
Abstract
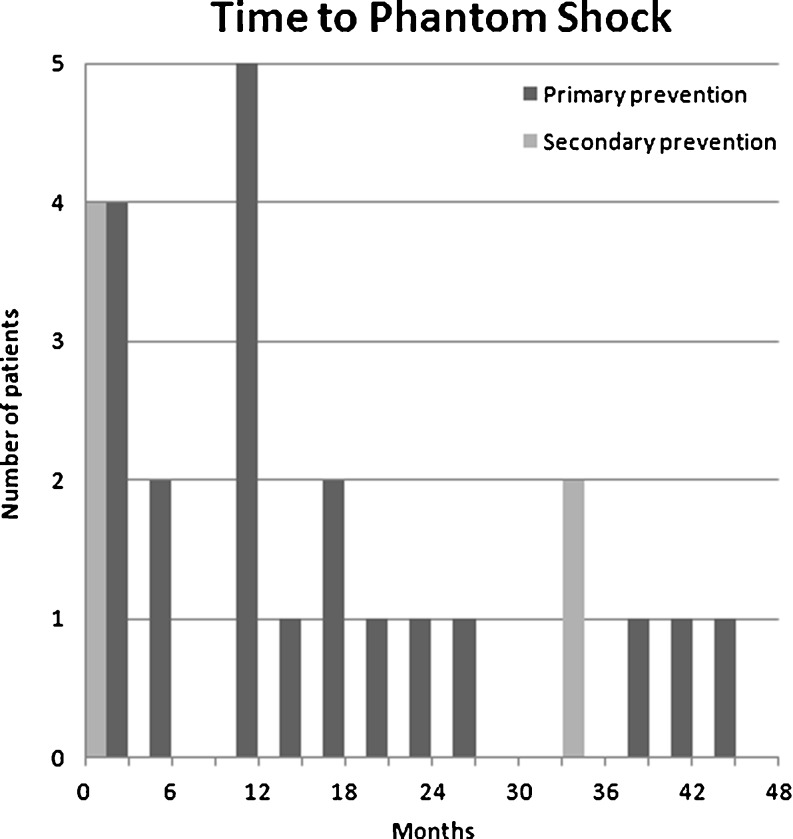
Background: Implantable cardioverter defibrillators (ICDs) are designed to deliver shocks or antitachycardia pacing (ATP) in the event of ventricular arrhythmias. During follow-up, some ICD recipients experience the sensation of ICD discharge in the absence of an actual discharge (phantom shock). The aim of this study was to evaluate the incidence and predictors of phantom shocks in ICD recipients.
Methods: Medical records of 629 consecutive patients with ischaemic or dilated cardiomyopathy and prior ICD implantation were studied.
Results: With a median follow-up of 35 months, phantom shocks were reported by 5.1 % of ICD recipients (5.7 % in the primary prevention group and 3.7 % for the secondary prevention group; p=NS). In the combined group of primary and secondary prevention, there were no significant predictors of the occurrence of phantom shocks. However, in the primary prevention group, phantom shocks were related to a history of atrial fibrillation (p=0.03) and NYHA class <III (p=0.05). In the secondary prevention group, there were no significant predictors for phantom shocks.
Conclusion: Phantom shocks occur in approximately 5 % of all ICD recipients. In primary prevention patients, a relation with a history of atrial fibrillation and NYHA class <III were significant predictors for the occurrence of phantom shocks. In the secondary prevention patients, no significant predictors were found.
Figures
References
-
- Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114(10):e385–e484. doi: 10.1161/CIRCULATIONAHA.106.178233. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
