

Case reports: acetabular damage after mild slipped capital femoral epiphysis
- PMID: 23184672
- PMCID: PMC3676598
- DOI: 10.1007/s11999-012-2715-7
Case reports: acetabular damage after mild slipped capital femoral epiphysis
Abstract
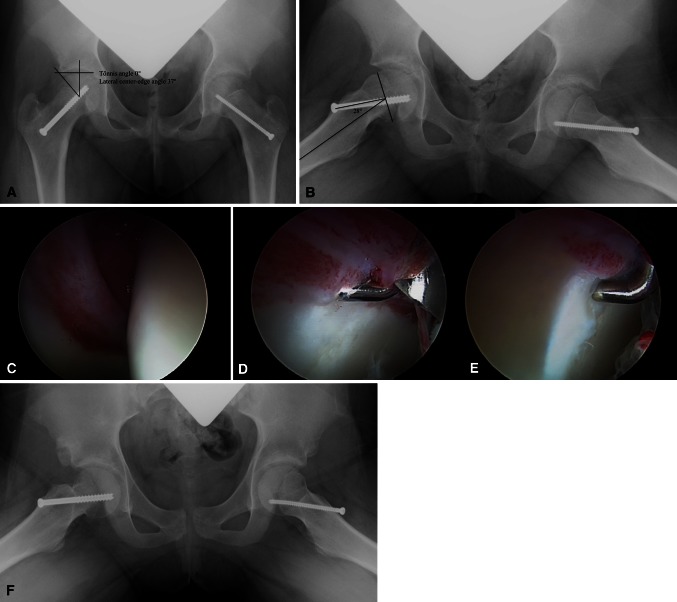
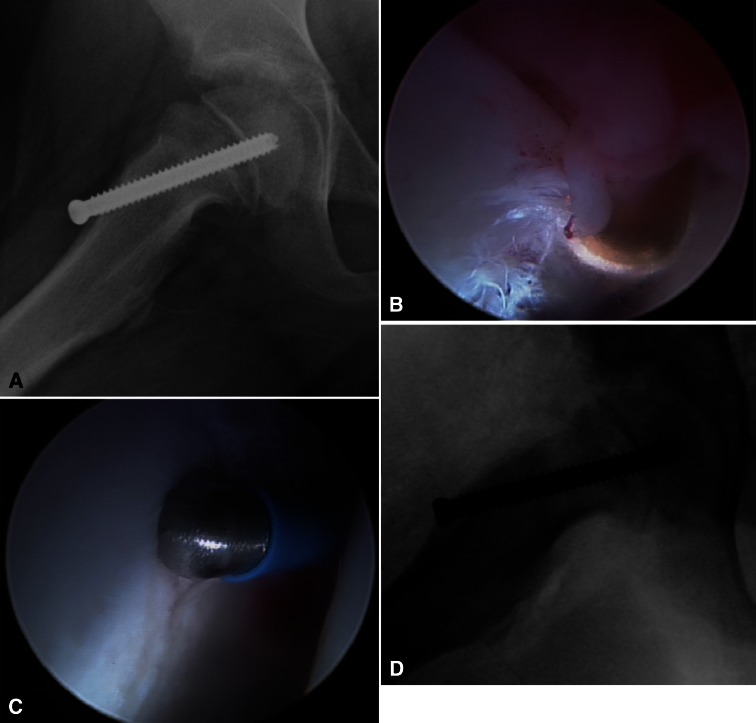
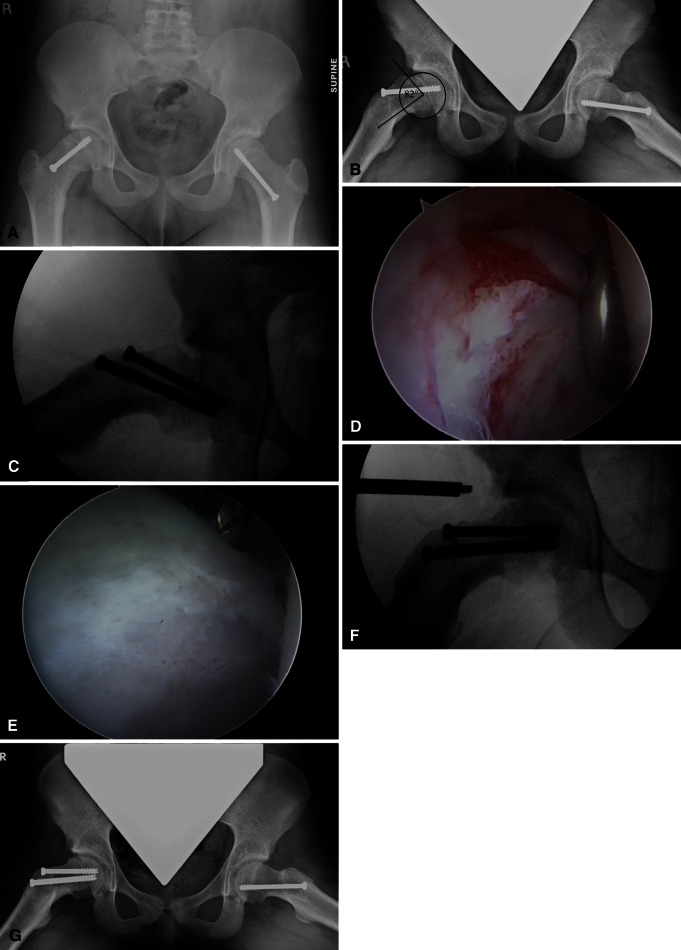
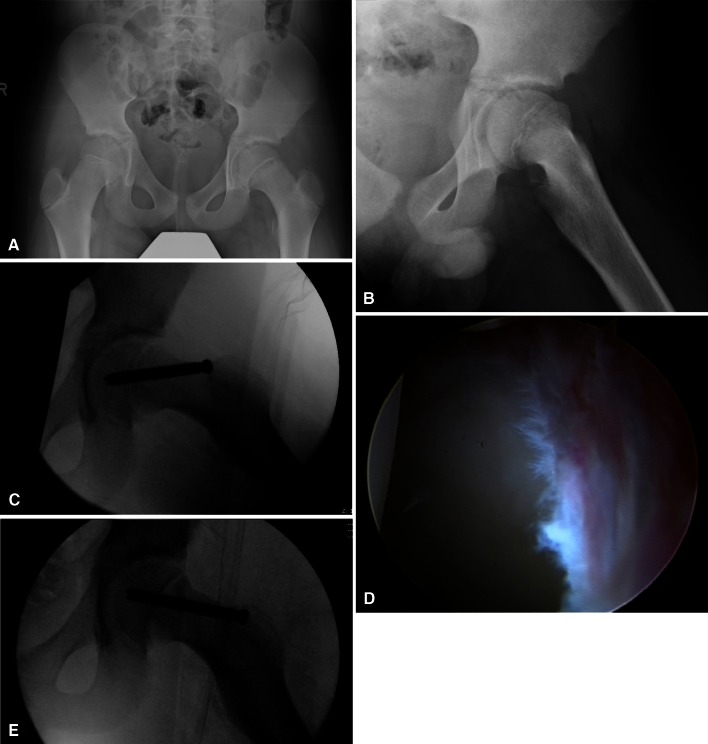
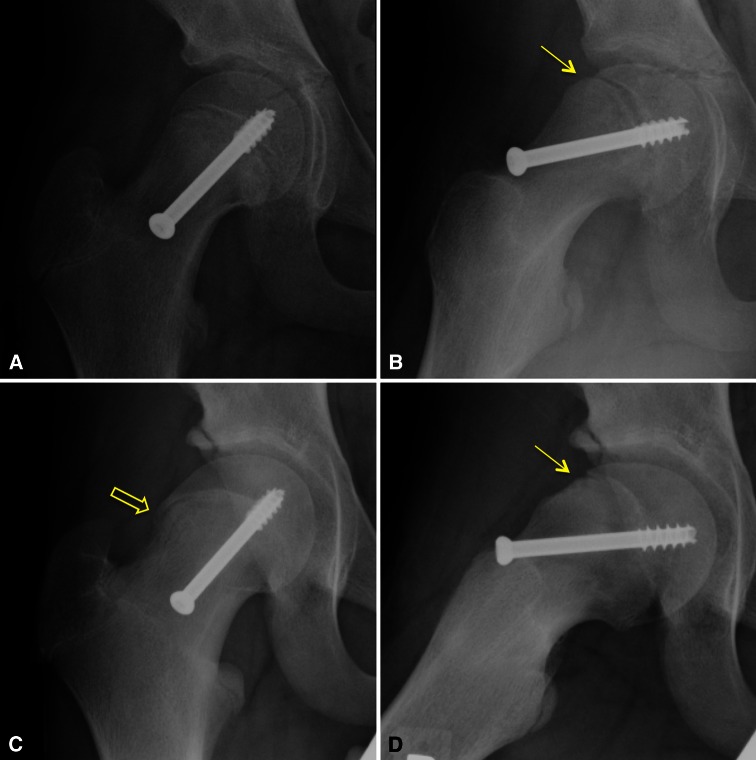
Background: Slipped capital femoral epiphysis (SCFE) is a common hip problem in adolescents that results in a cam-type femoroacetabular impingement (FAI) deformity. Although the treatment for mild (slip angle of 0°-30°) and moderate (slip angle of 31°-60°) SCFE has historically been in situ fixation, recent studies have demonstrated impingement-related articular damage, irrespective of slip severity. Our series confirms previous reports that acetabular chondral injury occurs in mild to low-moderate (slip angle of ≤ 40°) SCFE.
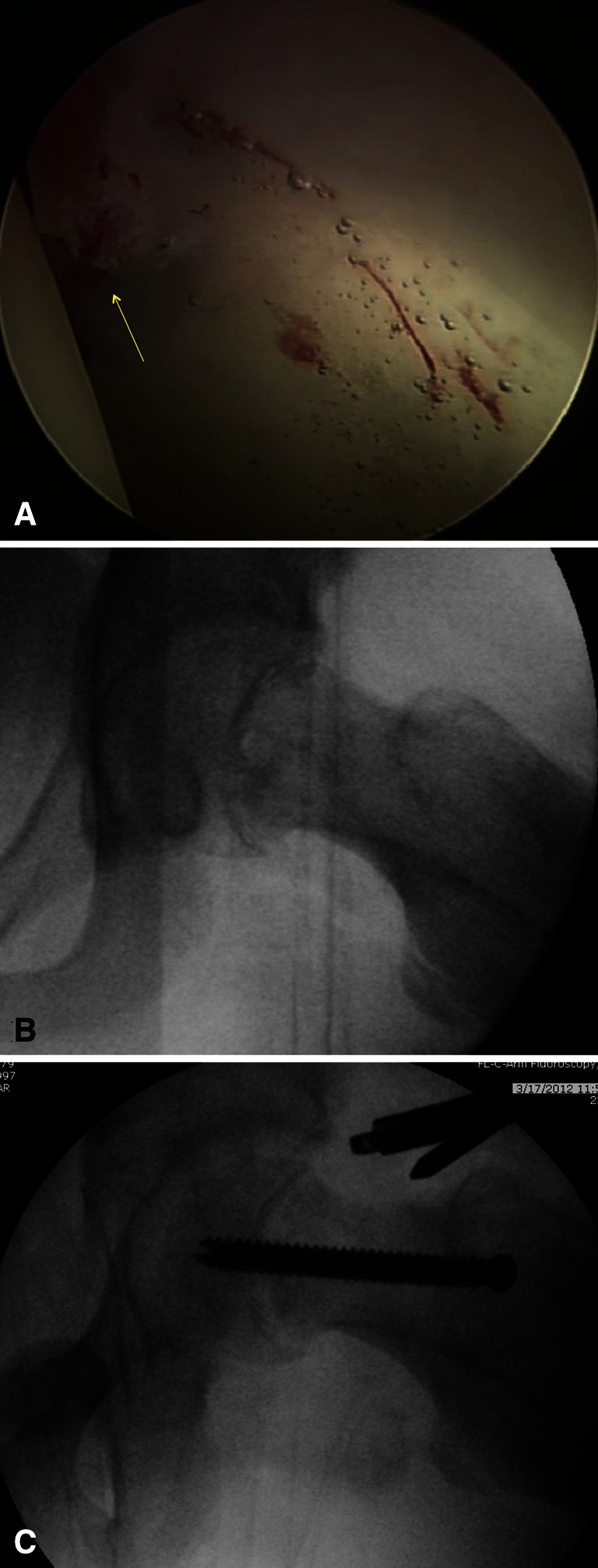
Case description: We retrospectively reviewed five patients who underwent arthroscopy and femoral osteoplasty within 18 months after in situ stabilization. All had labral and/or acetabular damage.
Literature review: Osteoarthritis rates after SCFE range from 24% to 92% at 11 to 28 years, depending on how osteoarthritis is defined. Long-term followup suggests patients have acceptable outcomes, but these studies are limited by heterogeneity and a ceiling effect from the instruments used to assess function. Although the femoral deformity remodels, it is unclear what secondary changes occur in the acetabulum. Recent investigations suggest patients are functionally limited after SCFE owing to FAI compared with controls. MRI findings and surgical reports document impingement-related joint damage after SCFE, even in the absence of symptoms. Based on this, some advocate timely correction of the cam deformity inherent in SCFE.
Purposes and clinical relevance: Further study is warranted to determine whether immediate osteoplasty after in situ fixation of mild SCFE is beneficial to limit articular damage and improve long-term outcomes.
Figures
Similar articles
-
Does a History of Slipped Capital Femoral Epiphysis in Patients Undergoing Femoroacetabular Osteoplasty for Femoroacetabular Impingement Affect Outcomes Scores or Risk of Reoperation?Clin Orthop Relat Res. 2021 May 1;479(5):1028-1036. doi: 10.1097/CORR.0000000000001576. Clin Orthop Relat Res. 2021. PMID: 33231940 Free PMC article.
-
Patients With Symptomatic Sequelae of Slipped Capital Femoral Epiphysis Have Advanced Cartilage Wear at the Time of Surgical Intervention.J Pediatr Orthop. 2021 Jul 1;41(6):e398-e403. doi: 10.1097/BPO.0000000000001797. J Pediatr Orthop. 2021. PMID: 33734202
-
Morphologic Features of the Contralateral Femur in Patients With Unilateral Slipped Capital Femoral Epiphysis Resembles Mild Slip Deformity: A Matched Cohort Study.Clin Orthop Relat Res. 2018 Apr;476(4):890-899. doi: 10.1007/s11999.0000000000000127. Clin Orthop Relat Res. 2018. PMID: 29481345 Free PMC article.
-
Slipped capital femoral epiphysis: what's new?Orthop Clin North Am. 2014 Jan;45(1):77-86. doi: 10.1016/j.ocl.2013.09.002. Orthop Clin North Am. 2014. PMID: 24267209 Review.
-
Slipped capital femoral epiphysis: prevalence, pathogenesis, and natural history.Clin Orthop Relat Res. 2012 Dec;470(12):3432-8. doi: 10.1007/s11999-012-2452-y. Clin Orthop Relat Res. 2012. PMID: 23054509 Free PMC article. Review.
Cited by
-
Risk factors for early symptomatic femoroacetabular impingement following in situ fixation of slipped capital femoral epiphysis.J Clin Orthop Trauma. 2022 Apr 1;28:101851. doi: 10.1016/j.jcot.2022.101851. eCollection 2022 May. J Clin Orthop Trauma. 2022. PMID: 35462635 Free PMC article.
-
The McMaster osteotomy-a novel surgical treatment to chronic slipped capital femoral epiphysis: description of surgical technique and case study.J Hip Preserv Surg. 2023 Nov 29;11(1):59-66. doi: 10.1093/jhps/hnad042. eCollection 2024 Jan. J Hip Preserv Surg. 2023. PMID: 38606328 Free PMC article.
-
Surgical treatment of symptomatic post-slipped capital femoral epiphysis deformity: a comparative study between hip arthroscopy and surgical hip dislocation with or without intertrochanteric osteotomy.J Child Orthop. 2020 Apr 1;14(2):98-105. doi: 10.1302/1863-2548.14.190194. J Child Orthop. 2020. PMID: 32351621 Free PMC article. Review.
-
Femoral and acetabular re-alignment in slipped capital femoral epiphysis.J Child Orthop. 2017 Apr;11(2):131-137. doi: 10.1302/1863-2548-11-170020. J Child Orthop. 2017. PMID: 28529662 Free PMC article.
-
Surgical treatment of femoroacetabular impingement following slipped capital femoral epiphysis: A systematic review.Bone Joint Res. 2017 Aug;6(8):472-480. doi: 10.1302/2046-3758.68.BJR-2017-0018.R1. Epub 2017 Aug 8. Bone Joint Res. 2017. PMID: 28790036 Free PMC article.
References
-
- Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87:1012–1018. - PubMed
-
- Boyer DW, Mickelson MR, Ponseti IV. Slipped capital femoral epiphysis: long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am. 1981;63:85–95. - PubMed
-
- Carney BT, Weinstein SL, Noble J. Long-term follow-up of slipped capital femoral epiphysis. J Bone Joint Surg Am. 1991;73:667–674. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
