

Development and validation of a composite programmatic assessment tool for HIV therapy
- PMID: 23185244
- PMCID: PMC3501505
- DOI: 10.1371/journal.pone.0047859
Development and validation of a composite programmatic assessment tool for HIV therapy
Abstract
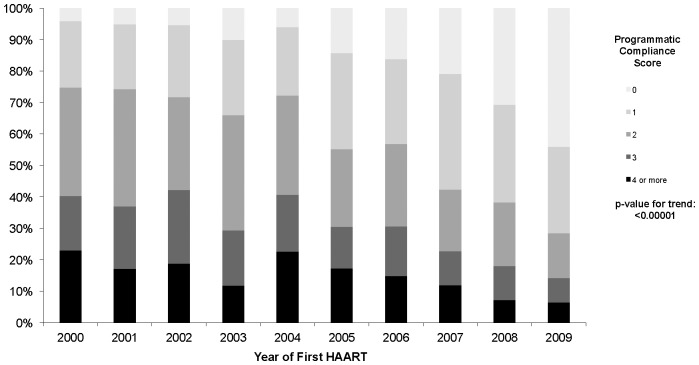
Background: We developed and validated a new and simple metric, the Programmatic Compliance Score (PCS), based on the IAS-USA antiretroviral therapy management guidelines for HIV-infected adults, as a predictor of all-cause mortality, at a program-wide level. We hypothesized that non-compliance would be associated with the highest probability of mortality.
Methods and findings: 3543 antiretroviral-naive HIV-infected patients aged ≥19 years who initiated antiretroviral therapy between January 1, 2000 and August 31, 2009 in British Columbia (BC), Canada, were followed until August 31, 2010. The PCS is composed by six non-performance indicators based on the IAS-USA guidelines: (1) having <3 CD4 count tests in the first year after starting antiretroviral therapy; (2) having <3 plasma viral load tests in the first year after starting antiretroviral therapy; (3) not having drug resistance testing done prior to starting antiretroviral therapy; (4) starting on a non-recommended antiretroviral therapy regimen; (5) starting therapy with CD4 <200 cells/mm(3); and (6) not achieving viral suppression within 6 months since antiretroviral therapy initiation. The sum of these six indicators was used to develop the PCS score - higher score indicates poorer performance. The main outcome was all-cause mortality. Each PCS component was independently associated with mortality. In the mortality analysis, the odds ratio (OR) for PCS ≥4 versus 0 was 22.37 (95% CI 10.46-47.84).
Conclusions: PCS was strongly associated with all-cause mortality. These results lend independent validation to the IAS-USA treatment guidelines for HIV-infected adults. Further efforts are warranted to enhance the PCS as a means to further improve clinical outcomes. These should be specifically evaluated and targeted at healthcare providers and patients.
Conflict of interest statement
Figures
References
-
- Carpenter CC, Fischl MA, Hammer SM, Hirsch MS, Jacobsen DM, et al. (1996) Antiretroviral therapy for HIV infection in 1996. Recommendations of an international panel. International AIDS Society-USA. JAMA 276: 146–154. - PubMed
-
- Carpenter CC, Fischl MA, Hammer SM, Hirsch MS, Jacobsen DM, et al. (1997) Antiretroviral therapy for HIV infection in 1997. Updated recommendations of the International AIDS Society-USA panel. JAMA 277: 1962–1969. - PubMed
-
- Carpenter CC, Fischl MA, Hammer SM, Hirsch MS, Jacobsen DM, et al. (1998) Antiretroviral therapy for HIV infection in 1998: updated recommendations of the International AIDS Society-USA Panel. JAMA 280: 78–86. - PubMed
-
- Carpenter CC, Cooper DA, Fischl MA, Gatell JM, Gazzard BG, et al. (2000) Antiretroviral therapy in adults: updated recommendations of the International AIDS Society-USA Panel. JAMA 283: 381–390. - PubMed
-
- Yeni PG, Hammer SM, Carpenter CC, Cooper DA, Fischl MA, et al. (2002) Antiretroviral treatment for adult HIV infection in 2002: updated recommendations of the International AIDS Society-USA Panel. JAMA 288: 222–235. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
